Download
1 / 10
110 likes | 433 Views
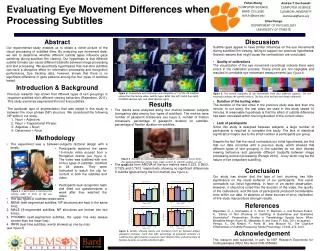
Horizontal eye movement. Generated from horizontal gaze center in PPRF which is connected to ipsilateral 6 th nerve nucleus. From 6 th CN nucleus internuclear neurons cross midline and pass to contralateral MLF to innervate medial rectus in the 3 rd nerve complex

E N D
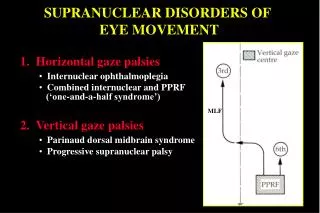
Horizontal eye movement • Generated from horizontal gaze center in PPRF which is connected to ipsilateral 6th nerve nucleus. • From 6th CN nucleus internuclear neurons cross midline and pass to contralateral MLF to innervate medial rectus in the 3rd nerve complex • Stimulation of PPRF on one side causes a conjugate movement of the eyes to the same side.
Vertical eye movements • Generated from vertical gaze center ( rostral interstitial nucleus of the MLF ) which lies in midbrain. • rostral interstitial nucleus of medial longitudinal fasciculus (riMLF) is a portion of the medial longitudinal fasciculus which controls vertical gaze.
medial longitudinal fasciculus (MLF) • It yokes the CN nuclei IIIand VI together, and integrates movements directed by the gaze centers (frontal eye field) and information about head movement. • t is an integral component of saccadic eye movements as well as vestibulo-ocular and optokinetic reflexes. • Lesions of the MLF produce internuclear ophthalmoplegia. Lesions to the MLF are very common manifestations of the disease Multiple sclerosis,where it presents as nystagmus and occasionally diplopia.
PPRF lesion gives rise to ipsilateral horizontal gaze palsy with inability to look in the direction of lesion. • MLF lesion gives rise to INO
Left INO • Straight eyes in primary position. • Defective left adduction. • Ataxic nystagmus of the right eye in right gaze. • Convergence is intact • Vertical nystagmus on attempted upgaze.
SUPRANUCLEAR DISORDERS OF EYE MOVEMENT 1. Horizontal gaze palsies • Internuclear ophthalmoplegia • Combined internuclear and PPRF • (‘one-and-a-half syndrome’) MLF 2. Vertical gaze palsies • Parinaud dorsal midbrain syndrome • Progressive supranuclear palsy
Internuclear ophthalmoplegia Lesion involving left MLF Normal left gaze Defective left adduction and ataxic nystagmus of right eye Convergence intact if lesion discrete Important causes • Demylination - usually bilateral • Vascular disease • Tumours of brainstem
‘One-and-a-half syndrome ’ Combined lesion of left MLF and PPRF • Defective left adduction • Ipsilateral (left) gaze palsy • Normal right abduction with ataxic • nystagmus
Parinaud dorsal midbrain syndrome • Supranuclear upgaze palsy • Normal downgaze • Large pupils with light-near dissociation • Convergence weakness • Lid retracton (Collier sign) • Convergence-retraction nystagmus Important causes • In children: aqueduct stenosis, meningitis and pinealoma • In young adults: demylination, trauma and a-v malformations • In elderly: vascular accidents and posterior fossa aneurysms
Progressive supranuclear palsy ( Steele-Richardson-Olszewski syndrome ) • Affects elderly • Pseudobulbar palsy Initially involves downgaze • Extrapyramidal rigidity • Gait ataxia • Dementia Subsequent defective up and horizontal gaze