Download
1 / 40
410 likes | 691 Views
The Knee Joint Complex. An overview of the structure and function of the knee joint complex. Lesley McLoughlin. Some pictures from slides have been removed to reduce file size Please refer to appropriate text book or Grey's anatomy. Content. Overview of the function of the knee joint complex

E N D
The Knee Joint Complex An overview of the structure and function of the knee joint complex. Lesley McLoughlin.
Some pictures from slides have been removed to reduce file size • Please refer to appropriate text book or Grey's anatomy
Content • Overview of the function of the knee joint complex • The tibio-femoral joint • Articular surfaces • The menisci • Ligaments • Bursae • Movements • Stability • The patello-femoral joint • Articular surfaces • Ligaments • Movements • Joint reaction forces • Stability
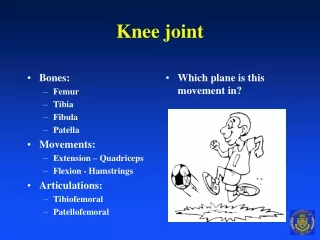
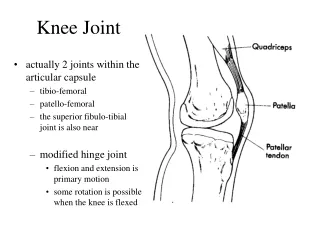
Overview • The joint between the two largest bones in the body • Allows functional shortening or lengthening of the lower limb • Works with the hip and ankle in a closed kinetic chain to support the body in dynamic and static activity • In an open kinetic chain it facilitates the mobility of the foot in space
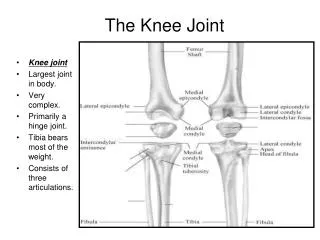
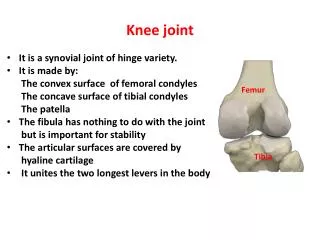
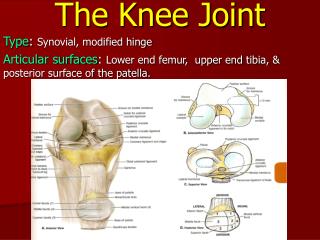
The knee joint complex • Type : compound / complex synovial • Two distinct articulations within one joint capsule : • Tibio-femoral - between the distal femur and the proximal tibia • Patello-femoral - between the patella and the femur
Tibio femoral joint : Articular surfaces • Incongruent • Femoral condyles • Bearing articular cartilage • Almost wholly convex • Lateral aspect; spiral with a curvature increasing posteriorly, the lateral condyle more rapidly
Tibio femoral joint :Articular surfaces Lateral aspect R distal femur
Tibio femoral joint : Articular surfaces • Tibial surfaces • Cartilage covered • Separated by the inter-condylar area • Gently hollow centrally • More flat peripherally where the menisci rest • Lateral; almost circular and smaller • Medial; more oval and larger
Tibio femoral joint : Articular Surfaces Superior surface R Tibia
Tibio femoral Joint : The menisci • Two semi lunar crescent shaped fibro-cartilages • Increase the congruency of the tibio femoral joint • Wedge shaped; thick peripherally and thin centrally • Each covers approximately 2/3 of its tibial surface • Aid weight distribution / shock absorption • Reduce friction
Almost a semi circle (an elongated C shape) Peripheral border is attached to the capsule and medial collateral ligament More firmly attached and therefore less mobile 4/5 of a circle (a closed C shape) Attached to the ACL Attached to the tendon of popliteus Fairly loosely attached as attachments are generally central this meniscus is therefore more mobile Medial Lateral
Meniscal ligaments • Posterior menisco femoral, (posterior attachment of the lateral meniscus to the medial femoral condyle) • Anterior menisco femoral, (posterior horn of the lateral meniscus to the medial femoral condyle) • Transverse genual, (anterior convex margin of the lateral meniscus to the anterior horn of the medial meniscus) • Coronary, (peripheral margins of the menisci to the superior surface of the tibia)
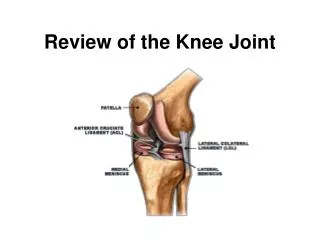
Tibio femoral joint : The menisci Transverse genual ligament Anterior cruciate Ligament Lateral Meniscus Medial Meniscus Posterior menisco femoral Ligament Posterior cruciate ligament
The knee joint complex :Ligaments • Have an important role in the stability and mobility of the knee joint complex • Close pack position : Extension Surfaces most congruent and ligaments are taut
The knee joint complex :Ligaments • Capsule • Complex • Deficient anteriorly • Augmented by thickenings in the capsule and expansions from adjacent musculature • Lined with synovial membrane
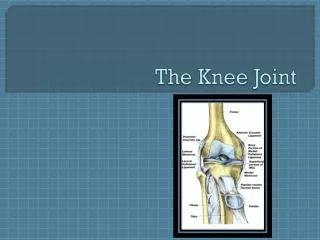
The knee joint complex :Ligaments • Tibial collateral ligament (medial) • Fibular collateral ligament (lateral) • Anterior cruciate ligament • Posterior cruciate ligament • Patellar ligament • Oblique popliteal ligament • Arcuate popliteal ligament
The knee joint complex :Ligaments Please refer to Williams, Warwick, Dyson & Bannister (1989)
The knee joint complex :Ligaments Please refer to Williams, Warwick, Dyson & Bannister (1989)
The knee joint complex:Bursae • Small sac lined with synovial membrane containing synovial fluid • Numerous (13) due to the extensive ligamentous and muscular support systems • Prevent friction between the various structures and therefore limit degenerative forces. • Some communicate with the joint capsule others are separate
The knee joint complex:Bursae Vertical section of the Left knee joint Please refer to Williams, Warwick, Dyson & Bannister (1989)
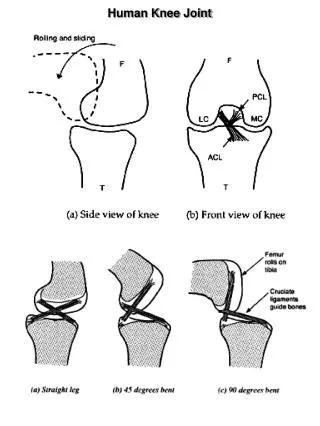
Tibio femoral joint:Movement • Physiological movements • Flexion • Extension • With the knee in some flexion, medial and lateral rotation The movements of flexion and extension are not pure hinge movements
Tibio femoral joint:Movement • The articulating surfaces of the femur are larger than those of the tibia • During flexion to extension if the femoral condyles purely rolled anteriorly they would run out of tibial condylar surface (Roll) • The femur must therefore glide posteriorly on the tibia as extension takes place (Glide)
Tibio femoral joint:Movement • As the medial condyle of the femur is larger than the lateral, the lateral condyle completes its rolling and gliding movements before the medial condyle. • This leads to a gradual conjunct medial rotation of the femur on the tibia (Spin and locking mechanism) • Conversely with the foot free the tibia laterally rotates on the femur
Tibio femoral joint:Movements of the menisci • In flexion the menisci are drawn backwards with the femur and are opened out transversely • In extension the menisci move forwards with the femur and are stretched more antero posteriorly to an oval shape • In axial rotation the menisci stay with the femur, the movement occurring between their lower surfaces and the tibial plateau
Tibio femoral joint:Movements of the menisci Flexion, menisci posterior and stretched transversely Extension, menisci anterior and stretched longitudinally
Tibio femoral joint :Stability • Shared between articular surfaces, ligaments and musculature • The articular surfaces with the help of the menisci remain incongruent • Even in the close pack position the surfaces only approach some element of congruency • Therefore a major contribution to stability is made by ligaments and muscles
Patello femoral joint • Type : Synovial Sellar • Least congruent joint in the body • The patella is the largest sesamoid bone in the body
Patello femoral joint:Articular surfaces • The patella surface on the femur • An inverted U on the anterior surface of both femoral condyles • Larger lateral than medial area • Concave transversely and convex vertically
Patello femoral joint:Articular surfaces Left Patellar surface on the femur
Patello femoral joint:Articular surfaces • The patella • Posterior surface covered in thick articular cartilage • Triangular shape • A vertical ridge divides the surface into larger lateral and smaller medial facets • Medial ‘odd’ facet
Patello femoral joint:Articular surfaces In flexion In extreme flexion In extension With infrapatellar fat pad Right patella
Patello femoral joint:Ligaments • Patellar ligament; the distal portion of the quadriceps tendon, from the apex of the patella to the tibial tubercle • Retinacular fibres from the VM and VL
Patello femoral joint:Movement • In extension the patella lies on a fat pad proximal to the trochlea • As flexion proceeds, the patella moves distally in the femoral trochlea groove • The track of the patella is C shaped, open laterally • As flexion begins the patella engages with the lateral trochlea wall and then with both the lateral and medial • As far as 90° flexion, the medial and lateral patellar facets only are engaged • At the extreme of flexion, the patella rotates about a vertical axis to bring the ‘odd’ facet into contact with the inner surface of the medial femoral condyle
Patello femoral joint:Functions • Creates an anatomical pulley. Increases the distance of the quadriceps tendon and patellar ligament from the knee joint axis, lengthening the moment arm and thereby altering the efficiency of the quadriceps Deflects the line of the quadriceps action away from the joint, increasing the angle of pull and the ability to generate torque • Reduces friction between the quadriceps tendon and the femoral condyles
Patello femoral joint:Reaction forces • The compressive force brought about by the pull of the quadriceps muscles and the patellar ligament • Occurs with both active and passive tension • Influenced by the magnitude of the pull and the angle of knee flexion
Patello femoral joint:Joint reaction forces (JRF) • Gait: at heel strike in 10° flexion the P/F. JRF = 50% body weight • Stairs: knee flexion 60° P/F. JRF = 3.3 x body weight • Squats; knee flexion 135° P/F. JRF = 7.8 x body weight • Reduced congruency as flexion increases means there is a reduction in joint compressive forces, hence medial facet degeneration is more common
Patello femoral joint:Stability • Longitudinal stability is provided by the quadriceps and the patellar ligament • Transverse stability is provided by the vasti and their retinacular fibres • Increased tension in the stabilisers can affect the sliding of the patella in the intercondylar groove (Patellar tracking) • Abnormal tracking can lead to tissue damage and clinical features such as pain and instability
Patello femoral joint:Stability • Due to the obliquity of the femur there is a mechanical tendency for the patellar to slip laterally. • This is prevented partly by the higher ridge of the lateral trochlea surface and by the pull of vastus medialis • However, if the lateral stabilisers become taut and the Vastus medialis becomes weak, the tracking of the patella is easily affected and the patella can become subluxed or even dislocated
The knee joint complex:Conclusion • A thorough knowledge of the structure and function of the knee joint complex will allow us to carry out a rigorous assessment and make a conclusive diagnosis, thereby enabling us to treat patients with knee pathologies and problems effectively
Bibliography • Williams,P.L., Warwick,R., Dyson,M & Bannister, L.H. (1989) Gray’s Anatomy • Norkin,C. & Levangie,P. (1992) Joint Structure and Function • Evans, P. (1986) The Knee Joint a clinical guide