Download
1 / 1
30 likes | 234 Views
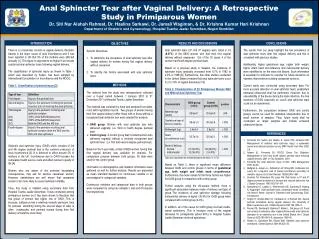
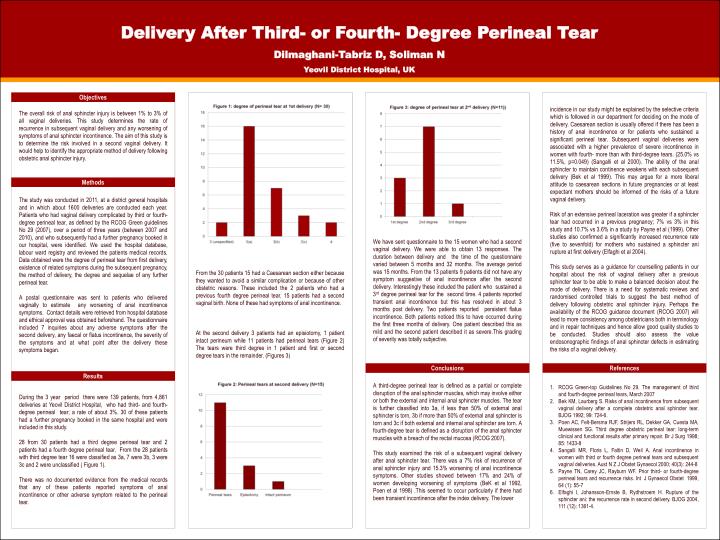
Delivery After Third- or Fourth- Degree Perineal Tear Dilmaghani-Tabriz D, Soliman N Yeovil District Hospital, UK.

E N D
Delivery After Third- or Fourth- Degree Perineal Tear Dilmaghani-Tabriz D, Soliman N Yeovil District Hospital, UK incidence in our study might be explained by the selective criteria which is followed in our department for deciding on the mode of delivery. Caesarean section is usually offered if there has been a history of anal incontinence or for patients who sustained a significant perineal tear. Subsequent vaginal deliveries were associated with a higher prevalence of severe incontinence in women with fourth- more than with third-degree tears. (25.0% vs 11.5%, p=0.049) (Sangalli et al 2000). The ability of the anal sphincter to maintain continence weakens with each subsequent delivery (Bek et al 1999). This may argue for a more liberal attitude to caesarean sections in future pregnancies or at least expectant mothers should be informed of the risks of a future vaginal delivery. Risk of an extensive perineal laceration was greater if a sphincter tear had occurred in a previous pregnancy; 7% vs 3% in this study and 10.7% vs 3.6% in a study by Payne et al (1999). Other studies also confirmed a significantly increased recurrence rate (five to sevenfold) for mothers who sustained a sphincter ani rupture at first delivery (Elfaghi et al 2004). This study serves as a guidance for counselling patients in our hospital about the risk of vaginal delivery after a previous sphincter tear to be able to make a balanced decision about the mode of delivery. There is a need for systematic reviews and randomised controlled trials to suggest the best method of delivery following obstetric anal sphincter injury. Perhaps the availability of the RCOG guidance document (RCOG 2007) will lead to more consistency among obstetricians both in terminology and in repair techniques and hence allow good quality studies to be conducted. Studies should also assess the value endosonographic findings of anal sphincter defects in estimating the risks of a vaginal delivery. Objectives The overall risk of anal sphincter injury is between 1% to 3% of all vaginal deliveries. This study determines the rate of recurrence in subsequent vaginal delivery and any worsening of symptoms of anal sphincter incontinence. The aim of this study is to determine the risk involved in a second vaginal delivery. It would help to identify the appropriate method of delivery following obstetric anal sphincter injury. Methods The study was conducted in 2011, at a district general hospitals and in which about 1600 deliveries are conducted each year. Patients who had vaginal delivery complicated by third or fourth-degree perineal tear, as defined by the RCOG Green guidelines No 29 (2007), over a period of three years (between 2007 and 2010), and who subsequently had a further pregnancy booked in our hospital, were identified. We used the hospital database, labour ward registry and reviewed the patients medical records. Data obtained were the degree of perineal tear from first delivery, existence of related symptoms during the subsequent pregnancy, the method of delivery, the degree and sequelae of any further perineal tear. A postal questionnaire was sent to patients who delivered vaginally to estimate any worsening of anal incontinence symptoms. Contact details were retrieved from hospital database and ethical approval was obtained beforehand. The questionnaire included 7 inquiries about any adverse symptoms after the second delivery, any faecal or flatus incontinence, the severity of the symptoms and at what point after the delivery these symptoms began. We have sent questionnaire to the 15 women who had a second vaginal delivery. We were able to obtain 13 responses. The duration between delivery and the time of the questionnaire varied between 5 months and 32 months. The average period was 15 months. From the 13 patients 9 patients did not have any symptom suggestive of anal incontinence after the second delivery. Interestingly these included the patient who sustained a 3rd degree perineal tear for the second time. 4 patients reported transient anal incontinence but this has resolved in about 3 months post delivery. Two patients reported persistent flatus incontinence. Both patients noticed this to have occurred during the first three months of delivery. One patient described this as mild and the second patient described it as severe.This grading of severity was totally subjective. From the 30 patients 15 had a Caesarean section either because they wanted to avoid a similar complication or because of other obstetric reasons. These included the 2 patients who had a previous fourth degree perineal tear. 15 patients had a second vaginal birth. None of these had symptoms of anal incontinence. At the second delivery 3 patients had an episiotomy, 1 patient intact perineum while 11 patients had perineal tears (Figure 2) The tears were third degree in 1 patient and first or second degree tears in the remainder. (Figures 3) Conclusions References Results • RCOG Green-top Guidelines No 29. The management of third and fourth-degree perineal tears, March 2007 • Bek KM, Laurberg S. Risks of anal incontinence from subsequent vaginal delivery after a complete obstetric anal sphincter tear. BJOG 1992; 99: 724-6. • Poen AC, Felt-Bersma RJF, Strijers RL, Dekker GA, Cuesta MA, Muewissen SG. Third degree obstetric perineal tear: long-term clinical and functional results after primary repair. Br J Surg 1998; 85: 1433-8 • Sangalli MR, Floris L, Faltin D, Weil A. Anal incontinence in women with third or fourth degree perineal tears and subsequent vaginal deliveries. Aust N Z J Obstet Gynaecol 2000; 40(3): 244-8 • Payne TN, Carey JC, Rayburn WF. Prior third- or fourth-degree perineal tears and recurrence risks. Int J Gynaecol Obstet 1999, 64 (1): 55-7 • Elfaghi I, Johansson-Ernste B, Rydhstroem H. Rupture of the sphincter ani: the recurrence rate in second delivery. BJOG 2004, 111 (12): 1361-4. A third-degree perineal tear is defined as a partial or complete disruption of the anal sphincter muscles, which may involve either or both the external and internal anal sphincter muscles. The tear is further classified into 3a, if less than 50% of external anal sphincter is torn, 3b if more than 50% of external anal sphincter is torn and 3c if both external and internal anal sphincter are torn. A fourth-degree tear is defined as a disruption of the anal sphincter muscles with a breach of the rectal mucosa (RCOG 2007). This study examined the risk of a subsequent vaginal delivery after anal sphincter tear. There was a 7% risk of recurrence of anal sphincter injury and 15.3% worsening of anal incontinence symptoms. Other studies showed between 17% and 24% of women developing worsening of symptoms (BeK et al 1992, Poen et al 1998) .This seemed to occur particularly if there had been transient incontinence after the index delivery. The lower During the 3 year period there were 139 patients, from 4,861 deliveries at Yeovil District Hospital, who had third- and fourth-degree perineal tear; a rate of about 3%. 30 of these patients had a further pregnancy booked in the same hospital and were included in this study. 28 from 30 patients had a third degree perineal tear and 2 patients had a fourth degree perineal tear. From the 28 patients with third degree tear 16 were classified as 3a, 7 were 3b, 3 were 3c and 2 were unclassified ( Figure 1). There was no documented evidence from the medical records that any of these patients reported symptoms of anal incontinence or other adverse symptom related to the perineal tear.