Download
1 / 39
400 likes | 672 Views
Glucocorticoids. Guochang Hu, MD, PhD Department of Pharmacology University of Illinois College of Medicine gchu@uic.edu. Knowledge Objectives 1. Synthesis, regulation and mechanisms of action 2. Physiological effects 3. Pharmacological effects 4. Glucocorticoid drugs

E N D
Glucocorticoids Guochang Hu, MD, PhD Department of Pharmacology University of Illinois College of Medicine gchu@uic.edu
Knowledge Objectives 1. Synthesis, regulation and mechanisms of action 2. Physiological effects 3. Pharmacological effects 4. Glucocorticoid drugs 5. Clinical uses 6. Side effects
Sites of Steroid Synthesis – Adrenal gland • Adrenal Medulla • Adrenal Cortex • ZonaGlomerulosa • ZonaFaciculata • ZonaReticularis Cortex Medulla
Sites of corticosteroid Synthesis – Cortex of Adrenal gland Mineralocorticoid Glucocorticoid Sex steroids
Diurnal Variation of Glucocorticoids % Change +100 Note: Related to sleep-Wake Cycle 8-10 am 0 -100 2 am 12 Midnight 12 Noon 12 Midnight LKS
Hypothalamic-Pituitary-Adrenal (HPA) Axis Feedback Cortico-centers • Amygdala – anterior brain - circadian rhythm • Reticular Formation – • Stressful stimuli CRH – Corticotropin releasing hormone ACTH – Adreno-corticotropic hormone ACTH binds receptors on surface of cells in zona fasciculata of adrenal cortex – cAMP second messenger increases production of glucocorticoid from cholesterol Glucocorticoid
Regulation of synthesis and secretion of adrenal corticosteroids The long negative feedback loop is more important than the short loop. Exogenous glucocorticoid negatively regulates synthesis and secretion of endogenous glucocorticoid CRH ACTH Daily administration of corticosteroid at physiological concentrations for at least 2 weeks suppresses the HPA resulting in decreased production of endogenous hormones. Recovery may take up to 9-12 months. ACTH has only a minimal effect on mineralocorticoid production. ADH, antidiuretic hormone (vasopressin)
Biosynthesis of corticosteroids and adrenal androgens Cholesterol Mineralocorticoid Metyrapone inhibits both glucocorticoid and mineralocorticoid synthesis. Aminoglutethimide and trilostane blocks synthesis of all three types of adrenal steroid.
Mechanism of Action • Enters target cells by simple diffusion • Binds to cytosolic receptors • The steroid receptor complex translocates into the nucleus • Regulates the synthesis of specific proteins
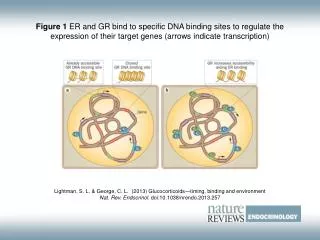
Steroid Receptor Activation S: steroid CBG: corticosteroid-binding globulin HSP: heat shock protein GRE: glucocorticoid response element
Glucocorticoid Receptor (GR) • Expressed in a almost every cell (cytosol) in the body and regulates genes controlling the development, metabolism, and immune response. • Associated with HSPs (e.g. HSP90) Upon activation by cortisol, GR translocates as a dimer (w/o HSPs) to nucleus Can also activate rapid signaling events in cytosol (non-genomic)
Target Tissues of Glucocorticoids Liver Skeletal Muscle Adipose Tissue Bone Brain Skin Retina Kidneys Heart Lymphoids Smooth Muscle Lung Stomach Intestines Fibroblast Testes = Most Important
Physiological Effects Direct receptor-mediated effects Indirect effects – homeostatic responses to other endogenous signals e.g. – increase blood glucose – increase in insulin
Physiological Effects 1. Metabolic Effects: Catabolic, glucose 2. Antiinflammatory and Immunosuppressive Effects 3. Other Effects
Metabolic effects Glucose Influence carbohydrate and fat metabolism to ensure adequate delivery of glucose to the brain Increase gluconeogenesis, decrease peripheral use of glucose Fat Increase in free fatty acids (increased lipolysis) Redistribution of fat from the extremities to the trunk and face (buffalo hump) Protein Favors protein breakdown and helps mobilize amino acids to the liver for gluconeogenesis
Anti-inflammatory and immunosuppressant activity Increase in circulating levels of neutrophils by interfering with adhesion Decrease in eosinophils, lymphocytes, and monocytes Decrease leukocyte migration, and phagocytic activity Decrease production of phospholipase A2, prostaglandins, thromboxanes and leukotrienes
Other Effects 1. Electolytes: Decrease absorption of Ca2+from the intestine and increase renal excretion of Ca2+ Increased Na+ and H2O reabsorption, increased K+ excretion. 2. Cardiovascular effects: Facilitates the effects of catecholamine, Maintenance of BP 3. Respiratory: Facilitates action of catecholamines (relax airway smooth muscle) Fetal lung maturation, increased surfactant secretion 4. Muscle: Maintain normal skeletal muscle 5. CNS Effects: mood, sleep patterns, and EEG
Pharmacokinetic Features • Well absorbed orally • Highly bound to plasma proteins (90%) - CBG • Metabolized by liver (P450 3A4 enzymes); excreted by kidney (75%) • Plasma half-life shorter than biological half-life • Substantial lag time before onset of action • Persistence of effect after disappearance from plasma
Pharmacological Effects (1) • Osteoporosis of Bone • Skin Thinning and Wasting • Connective Tissue Breakdown • Blood Changes • Neutrophils & Thrombocytes & RBC’s • Lymphocytes & Eosinophils & Basophils • CNS Effects: Mood Stability, Psychoses, • Excitability • H2O Retention
Pharmacological Effects (2) Suppressed Immune Response--Antiinflammatory Reaction Destruction of Eosinophils Stabilization of Lysosomal Membranes Inhibition of Arachidonic Metabolism Lipocortin (annexin) production Phospholipase A2 Prostaglandins & Prostacyclins & Leucotrienes Vasoconstriction and loss of Edema
Molecular mechanism of Anti-inflammatory effect A. Transactivation mechanism: up-regulate the expression of anti-inflammatory proteins (lipocortin I). B. Transrepression mechanism: down-regulate the expression of proinflammatory proteins (NF-кB, Fos, IL-1, TNF- α) transcription factors (TF). Transcriptional machinery (TM)
Mechanism of Anti-Inflammatory Effect Suppress T-cell activation and cytokine production Suppress mast cell degranulation Decrease capillary permeability indirectly by inhibiting mast cells and basophils Reduce the expression of cyclooxygenase II and prostaglandin synthesis Reduce prostaglandin, leukotriene and platelet activating factor levels by altering phospholipase A2 activity
of Effects on cytokines and Inflammatory Mediators
Comparison of Corticosteroids Differences between glucocorticoid drugs are potency, duration of action of the base, and pharmacokinetic behavior of the salts. • Stronger potency • Lower dose • Longer duration Synthetic Drugs
Clinical Uses of Glucocorticoids • Replacement Therapy • Anti-Inflammatory • Immuno-suppression • Treatment of Allergic Disorders
Glucocorticoid Insufficiency (Addison’s Disease) • Low adrenal activity • Hypoglycemia, hypotension, weakness, anorexia, irritability • Hyperpigmentation, hyperkalemia, hyponatremia
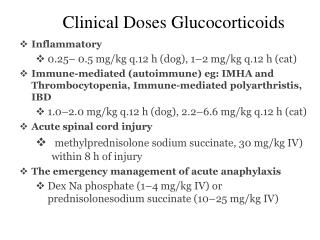
Arthritis Allergic reactions Asthma Autoimmune diseases Collagen disease Collagen vascular diseases – polymyalgiarheumatica, temporal arteritis Nephrotic syndrome Prevention of graft rejection (transplant) Dermatological disorders Respiratory distress syndrome Glucocorticoids – Uses for diseases
Side Effects Adrenocortical insufficiency: Suppression of HPA Adrenocortical excess (Cushing’s disease): “Moon face”, “buffalo hump” Diabetes Mellitus CNS effects: psychological and behavioral changes; aggravation of pre-existing psychiatric disorders Impaired wound healing Musculoskeletal effects: osteoporosis (brittle bones), muscle weakness and atrophy Cardiovascular effects: fluid retention, edema, hypertension
Cushing’s Syndrome • Hyper-Adrenalism • Primarily the Glucocorticoids
Side effects –impaired release of GH and decreased activity of insulin-like growth factor-1 (IGF-1) in growing bone
Withdrawal • “Cold turkey” if glucocorticoid therapy of less than 2 weeks duration • Taper off if Glucocorticoid therapy of greater than 2 weeks duration. • Rate of taper should be proportional to duration of prior therapy. • The longer the original therapy, the slower the rate of dose reduction. • Withdrawal syndrome: hypotension, hypoglycemia, myalgia and fatigue, joint pain, muscle stiffness, muscle tenderness, or fever.