Download

1 / 47
470 likes | 485 Views
Explore the milestones in immunization history, from Edward Jenner's smallpox vaccine to modern vaccines like HPV. Learn about vaccine biology, administration, and the national immunization schedule. Discover the importance of vaccination and immunization programs for disease prevention.

E N D
Milestones in immunization • 1780AD • Edward Jenner discovers small pox vaccine
Modern era of the vaccine • 1885 • Rabies vaccine (Pasteur) • 1934 • Pertussis • 1955 • Salk polio • 1920s • Diphtheria and Tetanus
Modern era of the vaccine • 1960s • Mumps measles and rubella virus • Sabin polio • 1985 • Haemophilus • 1990s • Hepatitis and varicella • 2000 Human Papillomavirus (HPV)
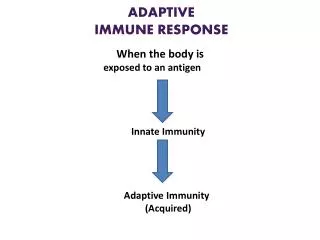
Vaccines Vaccines are whole or parts of microorganisms administered to prevent an infectious disease
Childhood immunization program is one of the best in the world. Free vaccines are provided to protect the baby against these 14 diseases: • Diphtheria Rotavirus Pneumococcal disease • Pertussis Hepatitis B Varicella • Tetanus Measles • Polio Mumps • Influenza Rubella • Haemophilus influenzae type B • Meningococcal disease
chemical modification toxin moiety antigenic determinants Modification of Toxin to Toxoid Toxin Toxoid
Immunization schedule For Government Programs it is cost first, efficacy next, safety last For Individual it is safety first, efficacy next, cost last
The following are alsoNOTcontraindications to vaccination: • Family history of any adverse reactions following immunisation • Previous history of pertussis, measles, rubella or mumps infection • Prematurity: immunisation should not be postponed • Stable neurological conditions such as cerebral palsy and Down’s syndrome • Contact with an infectious disease • Asthma, eczema, hay fever or ‘snuffles’ • Treatment with antibiotics or locally-acting (e.g. topical or inhaled) steroids • Child’s mother is pregnant • Child being breast fed • History of jaundice after birth • Under a certain weight • Over the age recommended in immunisation schedule • ‘Replacement’ corticosteroids
Influenza vaccine Meningococcal vaccine Cholera vaccine Rabies vaccine Yellow fever vaccine PPSV 23 HIGH-RISK children Recommended vaccines for HIGH-RISK children (Vaccines under special circumstances) • High-risk category of children: • Congenital/acquired immunodeficiency • Chronic cardiac, pulmonary, hematologic, renal, liver disease & diabetes mellitus • Children on long term steroids, salicylate, immunosuppressive or radiation therapy • Cerebrospinal fluid leak, Cochlear implant, Malignancies • Children with functional/anatomic asplenia/hyposplenia • During disease outbreaks • Laboratory personnel & health care workers • Travelers
Vaccine Administration • Preparation • Injection technique • Choice of needle length and size • Injection site These are all important considerations as each factor can affect both theimmunogenicity and the risk of local reactions at the injection site
Reconstitution of vaccine • Each vaccine should only be reconstituted and drawn up when required in order to: • Avoid errors • Maintain efficacy and stability • Reconstitution of freeze-dried vaccines: • -Only use diluent supplied and use within specified time period • -Only mix vaccines that are licensed and recommended to be mixed with other vaccines • -Diluent should be drawn up using a green (21G) needle and added slowly to vaccine to avoid frothing • Before administration: • -Check colour and composition of vaccine is as specified in description in vaccine’s • -Check vaccine to ensure is right product and correct dose for patient • -Check expiry date
Route of Injection • Vaccines should not be given intravenously • Most vaccines* should be given intramuscularly: • This reduces the chance of local reactions and leads to a better immune response to the vaccine • It is important the vaccine is injected into muscle and not into fat. This is why the deep subcutaneous route is no longer recommended for most vaccines • However: • Individuals with a bleeding disorder should receive their vaccines by deep subcutaneous injection to reduce risk of bleeding • *exceptions are BCG (intradermal injection), Japanese Encephalitis & Varicella vaccines (subcutaneous injection) and Cholera vaccine (oral)
Skin cleaning • Clean skin does NOT require cleaning • Visibly dirty skin need only be washed with soap + water • If alcohol and other disinfecting agents are used, skin must be allowed to dry as these could inactivate live vaccines
Positioning of Patient • All ages:ensure vaccination area is completely exposed • Babies and young children: • sit child sideways on parent’s lap • ensure child is held securely • if anterolateral aspect of thigh being used: parent to ‘cuddle’ child closely and place child’s nearest arm around parent’s back. Parent to place one of their arms over child’s other arm and hold both legs firmly by placing their hand just above the child’s knees • if deltoid being used: parent to hold arm to be injected close to child’s body and tuck other arm behind parent’s back. Tuck child’s legs between parent’s legs or ask parent to hold legs firmly
Screening for contraindications and precautions to vaccination • Is the child sick today? • Does the child have allergies medications, food, or any vaccine? • Has the child had a serious reaction to a vaccine in the past? • Has the child had a seizure, or brain or nerve problem? • Has the child a health problem with asthma, lung disease, kidney disease, metabolic disease such as diabetes, or a blood disorder?
Screening for contraindications and precautions to vaccination (Continue) • Does the child have cancer, leukemia, ADIS, or any other immune system problem? • Has the child taken cortisone, prednisone, other steroids, or anticancer drugs, or had x-ray treatments in the past 3 months? • Has the child received a transfusion of blood or blood products, or been given a medicine called immune (gamma) globulins in the past year? • Is the child/pregnant pregnant or there is a chance she could become pregnant during the next month? • Has the child received vaccination in the past 4 weeks?
Documentation • Date of administration • Title of vaccine(s) administered • Batch number • Expiry date • Site(s) of administration • Information as appropriate to record • Patient-held record
Consent • Consent must always be obtained before every immunisation its include: • What immunisation(s) are to be given • Which disease(s) will be prevented • Benefits and risks of immunisation versus risks of disease(s) • Possible side effects and how to treat • Any follow-up/action required • Any new information • Agreement to proceed
Deep freezer (-15 to -25O C) for ice packs & OPV stock for 3 months ILR (+2 to +8OC) BCG, DPT, DT, TT, measles, Hep B stock for 3 months Cold box (+2 to +8OC) for transport & power failure Vaccine carrier (+2 to +8OC) For 12 hours Cold chain
Vaccine Stability MOST SENSITIVE LEAST SENSITIVE • Sensitivity toHEAT BCG Varicella MMR MenC Hepatitis B DT and/or aP/IPV/HIB • Sensitivity to COLD HepB and combination DTand/or aP/IPV/HIB Influenza MenC *MMR *Varicella *BCG (*Freeze dried)
Light Sensitive Sensitive to strong light, sunlight, ultraviolet, fluorescents (neon) BCG MMR Varicella Meningococcal C Conjugate Most DTaP containing vaccines Vaccines should always be stored in their original packaging until point of use to protect them from light
Temperature Monitoring • Use max/min thermometer • Probe should be placed in the centre of fridge • Temperature should be recorded at least once a day • Reset daily • Calibrate as recommended • Take immediate action if temperature is outside recommended range
Sample refrigerator temperature record chart Available at: http://www2.cdc.gov/nip/isd/immtoolkit/content/vacstorage/logs.htm
Storage temperature Never exceed 8ºC or fall below 2ºC Aim for 5ºC • Aim to maintain vaccine fridge as close as possible to 5˚C as this gives a safety margin of + or – 3˚c
FACULTY OF NURSING UNIVESITY OF JORDAN