Download
1 / 41
410 likes | 614 Views
Human Subjects Studies. Unit of observation. Group (eg, geographic area). Individual. Cohort Cross-sectional Case-Control. Clinical Trial. Ecological Studies. Three Keys to Study Design Using Observation of Individuals. Identify the population that is the Study Base

E N D
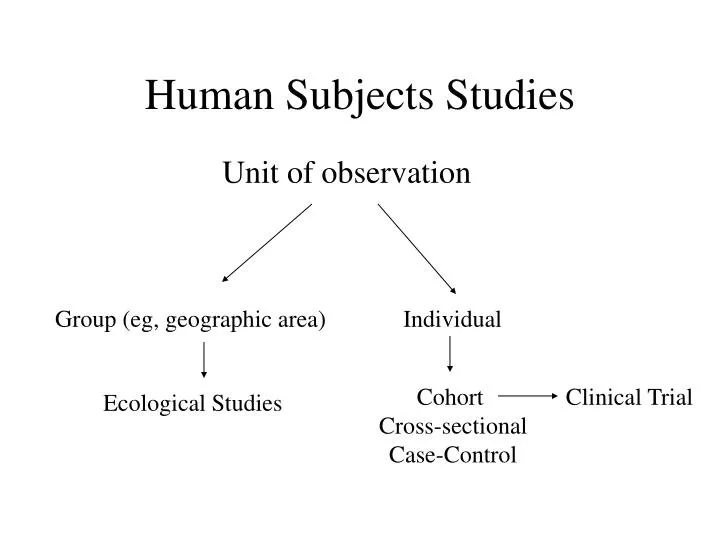
Human Subjects Studies Unit of observation Group (eg, geographic area) Individual Cohort Cross-sectional Case-Control Clinical Trial Ecological Studies
Three Keys to Study Design Using Observation of Individuals • Identify the population that is the Study Base • Determine how the experience of the Study Base population will be sampled • Consider the timing of measurements relative to the time period of the experience of the Study Base
Concept of the Study Base • The study base is the population who experience the disease outcomes you will observe in your study • In a cohort study, the study base is an explicitly defined cohort • In a cross-sectional study, the study base is a hypothetical cohort sampled at one point in time • In a case-control study, the study base is the cohort, either explicit or hypothetical, that gave rise to the cases
Cohort as the Basis of Design All study design is best thought of as ways of sampling the disease experience of a cohort
Cohort Study Design • Mimics individual’s progress through life and accompanying disease risk • Gold standard because exposure/risk factor is observed before the outcome occurs • Randomized trial is a cohort design with exposure assigned rather than observed • Case-control design, in particular, is best understood by considering how the experience of a cohort is sampled
Cohort study design D = disease occurrence; arrow = losses to follow-up Minimum loss to follow-up (1%)
Framingham Cohort Study The impact of diabetes on survival following myocardial infarction in men vs women. The Framingham Study.Abbott RD, Donahue RP, Kannel WB, Wilson PW. The impact of diabetes on recurrent myocardial infarction (MI) and fatal coronary heart disease was examined in survivors of an initial MI using 34-year follow-up data in the Framingham Study. Among nondiabetic patients, the risk of fatal coronary heart disease was significantly lower in women compared with men (relative risk, 0.6). In the presence of diabetes, however, the risk of recurrent MI in women was twice the risk in men. In addition, the effect of diabetes doubled the risk of recurrent MI in women (relative risk, 2.1) but had an insignificant effect in men. JAMA, 1989
Main Threat to Validity of a Cohort Study • Subjects lost during follow-up • Prospective cohort thought of as best study design but poor follow-up can change that • Equally true of clinical trials and observational cohorts • Number of losses is less important than how losses are related to outcome and risk factor
Subjects lost during follow-up • If losses are random, only power is affected • If disease incidence is research question, losses related to outcome bias results • If association of risk factor to disease is focus, losses bias results only if related to both outcome and the risk factor
Crucial issue is who is leaving cohort: What bias do the losses to follow-up introduce? Are disease diagnoses being missed? Are those with a risk factor more likely to leave and then be diagnosed? ? ? ? ? ? ? ?
Swiss HIV Cohort 3111 patients, ‘96-’99 At least two visits Med. follow-up 28 mos HCV+ more rapid disease progression Adj RH = 1.7 (95% CI = 1.3 - 2.3) No loss to follow-up info (Greub, Lancet, 2000) Johns Hopkins Cohort 1955 patients, ‘95-’01 At least two visits Med. follow-up 25 mos HCV not associated with disease progression Adj RH = 1.0 (95% CI = 0.9 - 1.2) No loss to follow-up info (Sulkowski, JAMA, 2002) Two Cohort Studies of HCV/HIV Coinfection and Risk of AIDS
Cross-Sectional Design • Measures prevalence of disease at one point in time. Two types: • Point prevalence: Do you currently have a backache? (study takes 4 months) • Period prevalence: Have you had a backache in the past 6 months? (study takes 4 months) • Main weakness: Cannot determine whether putative cause preceded the disease outcome
Case-Control Design: Concept of the Study Base • Study Base = the population that gave rise to the cases (Szklo and Nieto call it the “reference population”) • Key concept that shows the link between case-control design and cohort design
Case-Control Key Concept #1 • Think of the selection of cases and controls as occurring from a cohort
Cohort study design D = disease occurrence; arrow = losses to follow-up Given that all the cases are diagnosed, how would you sample controls from this cohort for a case-control study?
Three Ways to Sample Controls within a Cohort • At time each case is diagnosed = incidence density sampling • A random sample of the cohort baseline = case-cohort design • From persons without disease at the end of follow-up = prevalent controls design • A case-control study conducted from within a cohort is called a “nested case-control study”
Incidence Sampling within a Cohort Study Study Base = Cohort In this example, controls are sampled each time a case is diagnosed.
Incidence Density Sampling • In text example, 4 cases occur at 4 different points in time giving rise to 4 risk sets of cases and controls • Controls for each case are selected at random in each risk set from cohort subjects under follow-up at the time (called incidence density sampling) • It follows from the random selection, that a control can later become a case • Results can be just as valid as using entire cohort.
Case-control design using prevalent controls atend of follow-up.
Definition of a Primary Study Base • Primary Study Base = population that gives rise to cases that can be defined before cases appear by a geographical area or some other identifiable entity like a health delivery system or a cohort study
Case-Control Key Concept #2 • Any well defined population can be thought of as a cohort that continues to recruit new subjects during the time period of the study
Examples of Primary Study Bases • Participants in Women’s HIV Cohort Study • Residents of San Francisco during 2002 • Members of the Kaiser Permanente system in the Bay Area during 2002 • Military personnel stationed at California bases during 2002
Case-Control Incidence Density Sampling in a Dynamic Primary Study Base • Use a population-based disease registry to identify all new cases of disease during a defined time period and at the time each new case is reported sample controls from current residents • Use the rolls of a health care organization and proceed as above
Incidence Density Sampling in a Primary Study Base (e.g., San Francisco County) Primary Study Base New residents D Incidence-density sampling in a specified population with new subjects entering
Example of case-control study with incidence density sampling The association between long-term use of NSAIDs and non-Hodgkin lymphoma (NHL) was examined …in an ongoing population-based case-control study in the SF Bay Area. Cases were identified using Surveillance, Epidemiology, and End Results registry data. …Controls were a random sample of persons identified by random digit dialing… resided in the same six counties as the casesat the time of diagnosis… frequency-matched to cases by sex, age, and county of residence to ensure that they were from the same study base as the cases. …After adjustment for age and sex, there was no consistent association between long-term use and NHL for all NSAIDs combined, aspirin, nonselective NSAIDs, and COX-2 inhibitors. Flick, et al. Use of NonsteroidalAntiinflammatory Drugs and Non-Hodgkin Lymphoma: A Population-based Case-Control Study.Am J Epidemiol 2006; Sept 1, 164:497-504.
Case-Control Studies from a Secondary Study Base • Secondary Study Base = population that gave rise to cases=those persons who would have been cases if they had disease diagnosed during the time period of study • Start with cases and then attempt to identify hypothetical cohort that gave rise to them • Difficult concept but crucial to case-control design outside a well defined population
Case Control Studies from a Secondary Study Base • Source of cases is often one or more hospitals or other medical facilities • Problem is identifying who would come to the facility if diagnosed with the disease • Careful consideration has to be given to factors causing someone to show up at that institution with that diagnosis
Primary vs. Secondary Base • Main problem with a primary base is often ascertainment of all cases • eg, no registry of all cases for many diseases by geographic area • Main problem with a secondary base is the definition of the base • eg, hospital-based case-control studies common but very difficult to determine the study base
Primary vs. Secondary Study Base • Important, under-emphasized aspect of case-control design • Primary study base case-control studies can be very strong design • Secondary study base often not explicitly recognized by researchers • Even when recognized is still source of many bad case-control studies
Secondary Study Base • Example: glioma cases seen at UCSF • Difficult because referrals come from many areas • One possible control group might be UCSF patients with a different neurologic disease • Patients from a similar tertiary referral clinic are another possible control group • Residents of the neighborhood of the case are another possibility
Case-Control Key Concept #3 • A biased control group is usually the result of the inability to identify a well defined secondary study base (or the result of ignoring the study base concept entirely)
Two Concepts to Distinguish • Primary versus Secondary study base focuses on identifying the source of the cases and controls • Incident versus Prevalent sampling refers to how the cases and controls are sampled (both types of sampling can be done either in a primary or a secondary study base)
Example of a case-control design using prevalent cases • Sampling glioma patients under treatment in a hospital during study period • Poor survival so patients in treatment will over-represent those who live longest • Nature of bias variable and not predictable
Case Control Key Concept #4 • Incident sampling of both cases and controls is preferable to prevalent sampling
A Comment on the Terms Prospective and Retrospective • Prospective and retrospective refer to when the study is done in relation to the study base experience (text uses concurrent and non-concurrent) • But the key issue for the strength of the design is when were the measurements made in relation to the study base experience
Case Control Key Concept #5 • Strength of design rests on accurate measurements made prior to the outcome, not whether it is cohort or case-control sampling
Example of Study Design Choice • Kaiser Research Division 1990 • Question: Does screening sigmoidoscopy prevent colon cancer deaths? • Design choices • Prospective cohort: incidence about 100 deaths per yr but only about 15% of colon cancers detectable by sigmoidoscopy—10 to 20 yrs • Retrospective cohort: Kaiser members in 18-year period--100,000’s of records to review • Case-control
Colon cancer deaths 1971-1988: 1712 Cases=colon ca deaths detectable by sigmoidoscopy: 261 4 controls per case Controls = alive and in Kaiser at time of matched CA death (incidence-density) Blinded review of prior 10 years of medical records Predictor=screening sigmoidoscopy (not incl sigmoidoscopy for indication) 8.8% of cases vs. 24.2% had prior screening sigmoidoscopy Case-Control Design
Critical Features of Good Case-Control Design • Clearly identifiable study base (preferably a primary study base) • Cases: all, or random sample, of incident diagnoses in the study base • Controls: an unbiased sample of study base to estimate exposure prevalence in non-cases • Measurements preferably based on records or stored biological samples rather than recall