Download
1 / 58
640 likes | 1.25k Views
Arterial Blood Gas INTERPRETATION Manuel Antonio Ko, MD Section of Pulmonary Medicine Department of Internal Medicine Makati Medical Center. Objectives. Learn how to systematically interpret Arterial Blood Gas results Identify the different causes of abnormalities in the ABG results

E N D
Arterial Blood Gas INTERPRETATION Manuel Antonio Ko, MD Section of Pulmonary Medicine Department of Internal Medicine Makati Medical Center
Objectives • Learn how to systematically interpret Arterial Blood Gas results • Identify the different causes of abnormalities in the ABG results • Problem solving exercises
Indications for Arterial Blood Gas Determination • Evaluate Ventilatory, Oxygenation, Acid Base and Oxygen carrying capacity of blood • Monitor severity and disease progression • Quantify patient’s response to therapeutic intervention and or diagnostic evaluation Respircare, 1992, 317
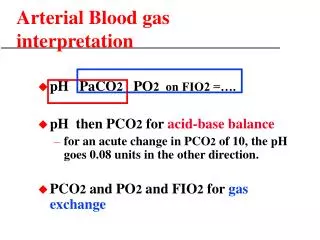
Steps in ABG Interpretation • Determine Acid Base Status (Acidotic or Alkalotic – pH Levels) • Identify the cause of the Acid Base Imbalance (Respiratory or Metabolic) • Determine compensation • Identify the Presence of Hypoxemia Correction of Hypoxemia • Report Interpretation
ABG Normal Values O2 Saturation 95 to 100 % Fio2 as indicated *a/A 0.8 * Not available in some ABG Machines
Neutral pH H+ / H2CO3 CO2 HCO3 Acidosis 7.35 7.4 7.45 Alkalosis Normal Range Normal or Compensated?
ABG Normal Values Base Excess – quick eye view of the adequacy of the buffer mechanism. If there is more than enough HCO3 to balance the pH (compensation)
Neutral pH H+ / H2CO3 CO2 HCO3 7.35 7.4 7.45 Normal Range Uncompensated or Partly Compensated Uncompensated or Partly Compensated Compensated Acidosis Alkalosis Increase PCO2 &/or Decrease HCO3 Decrease PCO2 &/or Increase HCO3
Compensation • Acute Respiratory Acidosis • PaCO2 increase by 10 mmHg decreases pH 0.08 • Bicarbonate increases 1 meq/L per 10 mmHg PaCO2 rise • Chronic Respiratory Acidosis • PaCO2 increase by 10 mmHg decreases pH 0.03 • Bicarbonate increases 4 meq/L per 10 mmHg PaCO2 rise
Acute Respiratory Acidosis Causes: 1. Central Nervous System Depression • Sedative Medications (e.g. Benzodiazepines) • Cerebrovascular Accident • Head Trauma 2. Neuromuscular Disease • Myasthenia Gravis • Guillain-Barre • Polio • Muscular Dystrophy • Hypokalemia 3. Impaired lung motion • Pleural Effusion • Pneumothorax • Crush injury
Acute Respiratory Acidosis Causes: 4. Acute airway obstruction • Foreign Body Aspiration • Tumor • Laryngospasm (e.g. Croup, Epiglottitis) • Bronchospasm (e.g. Asthma, COPD) 5. Acute Respiratory Disease • Severe Pneumonia • Pulmonary edema
Chronic Respiratory Acidosis Causes: • Chronic Obstructive Pulmonary Disease • Pickwickian Syndrome • Chronic Neuromuscular Disease • Thoracic cage limitation • Kyphoscoliosis • Scleroderma
Compensation • Acute Respiratory Alkalosis • PaCO2 decreases by 10 mmHg increases pH by 0.08 • Bicarbonate decreases 2 meq/L per 10 mmHg PaCO2 fall • Chronic Respiratory Alkalosis • PaCO2 decrease by 10 mmHg increases pH by 0.03 • Bicarbonate decreases 4 meq/L per 10 mmHg PaCO2 fall
1. Increased Central Respiratory Drive: • Anxiety • CNS Infection • Cerebrovascular Accident • Brain tumor • Head Trauma • Medications (Salicylates, Nicotine, Aminophylline, Progesterone, Cathecolamines) • Fever • Sepsis (especially with Gram Negative Bacteria) • Pregnancy • Liver failure, Cirrhosis or Hepatic Encephalopathy • Hyperthyroidism Respiratory Alkalosis Causes:
2. Increased Chemoreceptor Stimulation • Anemia • Carbon Monoxide Poisoning • Pulmonary edema • Pneumonia • Pulmonary Embolism • High altitude (decreased FIO2) • Restrictive lung disease (early) • 3. Iatrogenic with Mechanical Ventilation Respiratory Alkalosis Causes:
Compensation Metabolic Acidosis • PaCO2 decreased • PaCO2 drops 1.2 mmHg per 1 meq/L bicarbonate fall • Calculated PaCO2 = 1.5 x HCO3 + 8 (+/- 2) • Measured PaCO2 discrepancy: respiratory disorder • Useful in High Anion Gap Metabolic Acidosis
Metabolic Acidosis Elevated Anion Gap Acidosis • Anion Gap Definition • Difference between calculated serum anions and cations • Calculation • AG = Serum Na – (Serum Cl + Serum HCO3) • Interpretation • Normal Anion Gap: 12 +/- 2 meq/L
Metabolic Acidosis Elevated Anion Gap Acidosis (Mnemonic: "MUD PILERS")causes: • Methanol Intoxication • Uremia • Diabetic Ketoacidosis (DKA) or starvation ketosis • Paraldehyde, Phenformin • Isopropyl Alcohol, Isoniazid • Lactic Acidosis • Ethylene Glycol, ethyl alcohol • Rhabdomyolysis • Salicylates • Other Causes: Hyperalbuminemia, administered anions
Normal Anion Gap (Hyperchloremic Acidosis) A.) Hypokalemia with Metabolic acidosis: 1. Diarrhea/ Vomiting 2. Ureteral diversion • Uretero-sigmoidostomy • Ileal bladder • Ileal ureter 3. Renal Tubular Acidosis (proximal or distal) * 4. Mineralocorticoid Deficiency • Angiotensin Deficiency: Liver Failure • ACE Inhibitor • Renin Deficiency • Aging • Extracellular fluid volume expansion • Lead • Beta Blockers • Prostaglandin Inhibitor • Methyldopa 5. Carbonic Anhydrase Inhibitor • Acetazolamide • Mefenamic acid 6. Post-hypocapnia
Metabolic Acidosis Normal Anion Gap (Hyperchloremic Acidosis) B.) (Hyperkalemic or normal Potassium) Metabolic Acidosis 1. Renal Failure (Early)* 2. Renal Disease* • SLE Interstitial Nephritis • Amyloidosis • Hydronephrosis • Sickle Cell Nephropathy 3. Acidifying agents • Ammonium Chloride • Calcium Chloride • Arginine 4. Sulfur toxicity
Compensation Metabolic Alkalosis Serum HCO3 increased • PaCO2 increased • PaCO2 rises 6 mmHg per 10 meq/L bicarbonate rise • Expected PaCO2 = 0.7 x HCO3 + 20 (+/- 1.5) – discrepancy = Respiratory component • Excess Anion Gap >30 mEq/L
Metabolic Alkalosis Causes: A. Low Urine Chloride <10 meq/L 1.Gastrointestinal causes • Vomiting • Nasogastric suction • Chloride-wasting Diarrhea • Villous adenoma of colon 2. Renal Causes • Diuretic use (Urine Chloride <20 meq/L) • Poorly reabsorbable anion • Carbenicillin • Penicillin • Sulfate • Phsophate • Post-Hypercapnia
Metabolic Alkalosis Causes: A. Low Urine Chloride <10 meq/L 3.Exogenous alkali • Sodium Bicarbonate (baking soda) • Sodium Citrate • Lactate • Gluconate • Acetate • Transfusion • Antacid 4.Cystic Fibrosis 5. Achlorhydria 6. Contraction alkalosis
Metabolic Alkalosis Causes: B. Normal or High Urine Chloride >20 meq/L 1. Hypertensive Patient a. Adrenal Disease • Primary Hyperaldosteronism • Cushing's Syndrome (Pituitary, Adrenal or ectopic) • Liddle Syndrome b. Exogenous steroids • Excess mineralocorticoid intake • Excess glucocorticoid intake • Excessive licorice intake • Carbenoxalone • Glycyrrhizic acid • Chewing Tobacco 2. Normotensive Patient 1. Bartter Syndrome or Gitelman Syndrome 2. Hypokalemia 3. Excessive alkali administration 4. Milk-Alkali Syndrome 5. Refeeding alkalosis
Neutral pH H+ / H2CO3 CO2 HCO3 7.35 7.4 7.45 Normal Range Uncompensated or Partly Compensated Uncompensated or Partly Compensated Compensated Acidosis Alkalosis Increase PCO2 &/or Decrease HCO3 Decrease PCO2 &/or Increase HCO3
Oxygenation Status in ABG Report • Adequate Oxygenation at Given FiO2 - Pa02 = 80 to 100 mmHg • Hypoxemia at a Given FiO2 - PaO2 < 80 mmHg • More Than Adequate Oxygenation at a Given FiO2 - PaO2 > 100 mm Hg
Respiratory Components in ABG • PaO2 – Partial Pressure of Arterial Oxygen - NV: 80-100mmHG • PCO2 – Partial Pressure of Carbon Dioxide - NV: 35-45 mmHg • SaO2 – Oxygen Saturation in the Blood
SaO2 The oxygen-hemoglobin dissociation curve plots the proportion of hemoglobin in its saturated form on the vertical axis against the prevailing oxygen tension on the horizontal axis. It is usually a sigmoid plot. Hemoglobin molecules can bind up to four oxygen molecules in a reversible way. Many factors influence the affinity of this binding and alter the shape of the curve including: 1.) pH 2.) the concentration of 2,3-Diphosphoglycerate (2,3-DPG) 3.) the type of hemoglobin molecules (adult vs fetal types) 4.) the presence of poisons especially carbon monoxide
Hypoxemia in ABG • Inadequate oxygenation • Pa02 < 80 at a given level of FiO2 - FiO2 (Fraction of Inspired O2) - 21% at room air ( proportion of O2 in the atmosphere )
Respiratory Failure • Type 1 – Hypoxemia without CO2 retention (Normal PCO2) • ex.: Pulmonary Edema, Pneumonia • B. Type 2 – There is CO2 retention (Increased PCO2) • ex.: Hypoventilation (reduced alveolar ventilation) • pump failure, airway obstruction, neuromuscular • weakness • C. Combined
Determination of Hypoxemia (Parameters) 1. Partial Pressure of Alveolar Oxygen PAO2 2. Partial Pressure Difference between Alveolar and Arterial O2 A-aDO2 3. a/A Ratio (NV: 0.8) a/A ratio
A-aO2 Alveolar-Arterial Oxygen Tension Difference(PAO2 – PaO2) • PaO2 is generally lower than PAO2 - Physiologic shunt ( unoxygenated blood coming from the coronary arteries draining into the Thebesian Veins and parts of the Bronchial Arteries both draining directly into the Pulmonary Veins and bypassing the gas exchange mechanism of the lungs + diffusion of O2 to the alveolar capillaries) • Widens when there is pulmonary shunting (Pneumonia, edema & etc.). • Also widens when on supplemental oxygen ( more accurate when calculated at room air) • Minimal or no widening if the problem is pure hypoventilation 1
NORMAL PAO2 = 100 mmHg Alveolar PO2 (PAO2) Arterial PO2 (PaO2) Capillary PO2 O2 Diffusion through the Capillaries + Physiologic Shunt A-aDO2 PaO2 = 80-90mmHg (lower)
HYPOXEMIA Type 1 Resp. Failure PAO2 = 100 mmHg Alveolar PO2 (PAO2) Disease Arterial PO2 (PaO2) Capillary PO2 O2 Diffusion through the Capillaries + Physiologic Shunt + hypoxia Widened A-aDO2 PaO2 = 50 mmHg (much lower)
HYPOXEMIA PAO2 = inc. 300 mmHg Supplemental O2 Alveolar PO2 (PAO2) Disease Arterial PO2 (PaO2) Capillary PO2 O2 Diffusion through the Capillaries + Physiologic Shunt + hypoxia Widened A-aDO2 PaO2 = inc. 75 mmHg ( but slightly lower than normal)
HYPOVENTILATION Type 2 hypoxemia PAO2 already Decreased PAO2 = 60mm.Hg Hypoventilation Alveolar PO2 Arterial PO2 (PaO2) Capillary PaO2 PaO2 = 50 mm Hg – No significant widening of the AaDO2
Airway Obstruction HYPERCARBIA PACO2 = Decreased Hypoventilation Alveolar PCO2 (PACO2) Arterial or Mixed Venous PCO2 (PaCO2/ PVCO2) Capillary PCO2 Increase PCO2
Determination of Hypoxemia 1. Partial Pressure of Alveolar Oxygen PAO2 = PiO2 – PCO2/0.8 (PiO2 = 713 X FiO2) 2. Partial Pressure Difference between Alveolar and Arterial O2 A-aD02 = PAO2 – PaO2 3. a/A Ratio (NV: 0.8) a/A = PaO2/PAO2
O2 Correction Des. PaO2 / (a/A) + PCO2 / 0.8 Desired FiO2= ________________________ 713 1. Desired PaO2 – 80 to 100 mmhg 2. (713) – Atmospheric pressure – water vapor pressure [ constant ] 3. PCO2 – Partial Pressure Carbon Dioxide 4. (0.8) – Respiratory Quotient ( volume of CO2 produced/ volume of O2 consumed )[ constant ] 5. a/A – PaO2 (Arterial O2) / PAO2 (Alveolar O2)
P/F Ratio PaO2/ Fio2 (simple estimate) • Indicates range of hypoxemia • P/F ratio > or equal 400 - Normal • P/F ratio < 400 - Hypoxemia
Giving O2 Supplement • Supplemental O2 conversion -LPM Oxygen = LPM x 4 + 20 ( Fi02) ex: 2 (LPM O2) x 4 + 20 = 28% FiO2 (using O2 cannula, O2 mask) (O2 supplementation is not provided by direct FiO2)
Conditions invalidating or modifying ABG Results • A. Large Air bubbles not expelled from sample: • PaO2 rises 0-30 mmHg • PaCO2 may fall slightly • B. Fever or Hypothermia: • Patient temperature shifts oxy-hemoglobin curve • C. Hyperventilation or breath holding (due to anxiety):
Conditions invalidating or modifying ABG Results • D. Delayed analysis: • 1. Iced Sample maintains values for 1-2 hours 2. Un-iced sample quickly becomes invalid • PaCO2 rises 3-10 mmHg/hour • PaO2 falls at a rate related to initial value • pH falls modestly • E. Excessive Heparin: • Dilutional effect on results 2. Decreases bicarbonate and PaCO2
Case 1 • 65 year old male, seen at the ER, diagnosed case of Chronic Renal Failure presently undergoing Hemodialysis. He was placed on Multivent Mask at 40% FiO2. Chest X-ray shows Increase Broncho-vascular markings with concomitant interstitial and alveolar infiltrates on the Right Lower Lobe PPE: • T= 37.8, RR: 26, BP: 90/60, CR: 115 • Pale skin and Diaphoretic • Use of accessory muscle and abdominal breathing pattern observed • fine crackles on the right lower lung fields with expiratory wheezes all over • bipedal edema noted
Interpret Acid Base Status? • Determine if Hypoxemia Exists ? • Compute the a-AO2 gradient ? • Compute for the desired FiO2 ? • Compute Anion Gap ? • Initial Diagnosis? • What are your immediate plans for the patient ?
Acute Respiratory Acidosis Causes: 4. Acute airway obstruction • Foreign Body Aspiration • Tumor • Laryngospasm (e.g. Croup, Epiglottitis) • Bronchospasm (e.g. Asthma, COPD) 5. Acute Respiratory Disease • Severe Pneumonia • Pulmonary Edema
Metabolic Acidosis Elevated Anion Gap Acidosis • Anion Gap Definition • Difference between calculated serum anions and cations • Calculation • AG = Serum Na – (Serum Cl + Serum HCO3) • Interpretation • Normal Anion Gap: 12 +/- 2 meq/L