Download
1 / 26
280 likes | 304 Views
Explore the impact of prenatal substance exposure on children's health, development, and behavior and learn about an intervention program providing essential support. Discover the risks, effects, and diagnostic criteria associated with prenatal alcohol exposure.

E N D
Prenatal Alcohol and Drug Exposure SHELLEY HOUSTON, MEd LMHC April 11, 2013
Pediatric Interim Care (PIC) Program through Providence Regional Medical Center Everett (PRMCE) • Must have an open CPS case (can be voluntary or dependency case) • Must have documented alcohol or drug exposure in utero OR… be medically fragile with need for intensive case management services • Must be referred by CPS • Must be between birth and 3 years of age • Must be within Snohomish County • Monthly home visits, more frequent if needed • Up to 18 months of case management and nursing services by PIC Social Worker and RN
The difficulties obtaining clear outcomes of prenatal substance exposure • Even with prenatal history available, it is extremely difficult to disentangle the consequences of prenatal substance exposure from the frequent co-occurence of prematurity, malnutrition, neglect, abuse, multiple placements. In addition, prenatal exposure to potentially harmful substances often occurs in the context of social dysfunction: • poverty, • parental addiction, • impaired parenting, and • poor access to services. • A family history of mental illness or learning disabilities is often present, which can carry additional genetic risk for infants. With increasing poly drug abuse as well as use of tobacco, alcohol and prescribed drugs to pregnant women, it is becoming increasingly difficult to differentiate the effect of any single drug on the newborn infant.
Alcohol consumption during pregnancy is the leading cause of preventable birth defects & developmental problems • All leading health organizations agree that there is no safe time or safe amount of alcohol to use in pregnancy and recommend abstinence. • The timing and dose of alcohol use during pregnancy are important when considering potential implications for the developing fetus. Children born to women who drink heavily on a regular basis in the first trimester of pregnancy have the greatest risk of CNS damage. The first month of pregnancy is particularly crucial for development of the CNS and the midportion of the face. Unfortunately, this early in pregnancy, many women do not realize that they are pregnant and continue their usual pattern of alcohol ingestion. • low birth weight (LBW) and ‘‘mild’’ disability can be seen at an exposure of roughly 2 alcoholic drinks per day (lower in recent studies). • When 4 to 6 drinks are consumed, additional clinical features become evident. • Most of the children who are believed to have the full expression of FAS are born to women consuming 8 to 10 drinks or more per drinking occasion, on a regular if not daily basis, for at least the first trimester. It is estimated that the risk of a ‘‘serious problem’’ in the offspring of chronically alcoholic women ranges from 30% to 50%. The greatest risk is that of mental deficiency as well as a host of learning and behavioral disabilities [15].This could include problems with
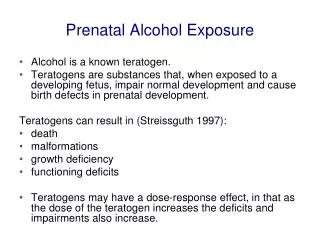
Prenatal Alcohol Exposure & Fetal Alcohol Spectrum Disorders • Alcohol presents more risk to the fetus than any other drug of abuse • Fetal alcohol spectrum disorders (or FASD) encompass the range of effects that might result from prenatal exposure to alcohol • FASD is not a clinical diagnosis but FASDs do include physical, mental, behavioral and learning disabilities. • Risks associated with prenatal alcohol exposure include: • Intrauterine growth deficiency • Abnormal facial features • Poor coordination • CNS damage, including intellectual diability or low IQ, learning disabilities (severe to undetectable), hyperactivity, and attention deficits, poor reasoning, poor judgment, poor academic achievement, and even insecure attachment • Alcohol is considered a teratogen because it causes defects to organs including the central nervous system, Heart, kidney and bone issues
Diagnostic Criteria for FAS(Fetal Alcohol Syndrome) • Growth deficiency • Cluster of facial anomalies, including a thin upper lip, a smooth philtrum (vertical groove between the nose and upper lip), and small palpebral fissure lengths (PFLs; width of eye openings) • Evidence of CNS (Central Nervous System) damage or dysfunction • History of maternal alcohol use during pregnancy • The 4-Digit Diagnostic Code 3444 inserted in the grid is one of twelve 4-Digit Codes that meet the diagnostic criteria for FAS. Courtesy of S. Astley, PhD, Seattle, WA
Prenatal alcohol exposure • Prenatal alcohol exposure early in pregnancy has been found to increase the likelihood of developing an alcohol disorder in adulthood • Research continues to find cognitive and socioemotional deficits among children exposed to even small amounts of alcohol • Alcohol–exposed children with supportive mothers cope better with frustration – the role of the home environment determines the effects of substance exposures on child outcomes
Alcohol exposure outcomes What helps these children? 1) Younger age at diagnosis Because: S/he • can be placed in appropriate educational classes • given access to social services that can help both child and family • helps families and school personnel understand why the child might act or react differently from other children in some situations 2) Life in a loving, stable and nurturing home: Children with FASD can be particularly sensitive to disruptions, transient lifestyles, or harmful relationships. Less likely to develop secondary conditions if they are not exposed to violence. 3) A structured predictable daily routine is helpful for many children with executive function difficulties (alcohol and marijuana exposed children)
Prenatal Opiate exposure: Heroin, Methadone, Oxycontin • Significant risk of preterm delivery; less so with methadone • Elevated risk for stroke while pregnant • Low birth weight – more so with heroin • 3-6 months old irritability and poor state control Possible longer term outcomes: • short attention span, • hyperactivity • Memory and perceptual problems and • sleep disturbances
Neonatal Abstinence Syndrome Central Nervous System Disturbances • High pitched cry or continuous cry • Hyperactive moro reflex • Mild or moderate or severe tremors • Hypersensitivity • Increased muscle tone • Excoriation • Myoclonic jerks – involuntary muscle spasms • Convulsions or seizures
Neonatal Abstinence Syndrome Metabolic, vasomotor, & respiratory disturbances • Sweating • Fever • Frequent Yawning – more that 3 times in 3 hours • Mottling – marbling of skin • Nasal Stuffiness • Sneezing – more than 3 times every 3 hours • Nasal Flaring • Rapid Breathing – over 60 breaths per minute (sometimes with retractions)
Neonatal Abstinence Syndrome Gastrointestinal Disturbances Disorganized suck/Frantic suck Excessive sucking Flatus – gas for more than 3 hours Poor Feeding Regurgitation Projectile Vomiting Loose Stools Water Ring Stools – has substance like mashed potates and a water ring surrounding the stool Loose Stools – curdy, seedy, or runny in appearance Watery Stools Blood in stool Hypersensitivity to feeds, touch, sound, smell, energy levels, surroundings, light, eye contact, movement
Prenatal Tobacco exposure • Miscarriage, placenta previa, abruption, premature rupture of membranes, preterm birth, intrauterine growth restriction and sudden infant death syndrome (SIDS) • Cleft lip anomalies • Low birth weight • Smaller head circumference at birth • Respiratory & ear infections, lung function & asthma Withdrawal effect/toxicity: • hyper tonicity (tight muscle tone) • Tremors • sucking difficulties • altered cries • Attention deficit hyperactivity disorder (ADHD)-like symptoms
Prenatal Tobacco/Nicotine exposure Long term: • Behavioral problems • Decreased IQ scores (average of 4 points lower) • Language delays • Coordination or physical control problems • Learning and memory problems • Impulsivity and attention problems • Hyperactivity and negative and externalizing behaviors in children which can continue in the form of higher rates of delinquency, criminal behavior and substance abuse
Prenatal Marijuana Exposure • Abnormal newborn behavior consistent with associated with narcotic exposure Long Term: • Reading and spelling academic difficulties • Memory and verbal abilities at 4 years old possibly are impacted by heavy prenatal exposure • Some impact on motor development, possibly fine motor or quality of movement • Poor problem-solving skills requiring visual integration, analysis and sustained attention • Inattention and/or impulsivity • Impact on higher level executive function & performance
Prenatal Cocaine Exposure • Stillbirth, preterm delivery, placental abruption, premature rupture of membranes • Small head size • Growth restriction with higher levels of exposure which could be due to not waking to feed and only eating small amounts at a time • No cocaine withdrawal syndrome but • irritability, excitability • lability of state, • decreased behavioral and autonomic regulation which can lead to poor feeding • Poor alertness and orientation • Strokes • Seizures
Prenatal Cocaine Exposure Long term effects: • OVERALL EXECUTIVE FUNCTIONING - Poor memory & information processing, working memory, attention, visual motor ability • Possible ADHD-like symptoms, attention processing, and oppositional defiant disorder reported by exposed children themselves • Preschool impulse control issues reported • At 3 years of age: increased fussiness, difficult temperament, behavior problems • Language delay has also been described • Some studies say there is no difference between the cocaine-exposed child and the non-exposed child in regards to cognition and child development which suggest that the physical and social environments of children may have a more significant impact on development than cocaine use alone
Prenatal Methamphetamine Exposure • Limited studies on fetal methamphetamine exposure • Most women who use meth also use alcohol and/or nicotine, it is difficult to determine effects of the methamphetamine alone Research to date states: • Smaller brain structures, cleft & cardiac anomalies • Premature delivery, Placental abruption • Lower birth weight; small for gestational age • Feeding difficulties the same as cocaine exposure Withdrawal symptoms similar to NAS sometimes • irritable, • poor eye contact, • lethargic, • muscle tone issues (low or high), • disorganized or no suck, • elimination of toxins • Used 1st trimester: signs of stress in infants • Used 2nd trimester: lethargy • Used 3rd trimester: poorer quality of movement
Methamphetamine Exposure Long term inconclusive: • Possible links with aggressive behavior, peer problems and hyperactivity • One study found that these children scored lower executive functioning: on visual motor integration, attention, verbal memory, and long-term spatial memory • No data available on language development POST-NATALLY EXPOSED CHILDREN Need medical assessment immediately and seek further medical attention if headache, drowsiness, unusual movements (tremors, shaking, agitation, seizures), trouble breathing, poor color, fever, hallucinations or mental confusion Decontamination procedures – thorough washing of child and clothes Traumatic environment – neglect, greater risk of abuse including sexual abuse, inadequate supervision, inconsistent parenting, exposure to second-hand smoke and ingestion of drug, exposure to HIV, Hep C, etc. from needles, chemical burns, undernourishment, respiratory problems, undernourishment, delayed physical development…
Common Symptoms of drug exposed babies Managing infants during withdrawal/toxicity period Environment: reduce stimuli, provide routine, use calming techniques Learn Baby’s Cues: Respond to distress cues (Yawns, sneezes, hiccoughs, tremors, color change, frowns, eye aversion) – if you see these stop what you are doing: these indicate overstimulation Calming Techniques: calm before infant reaches frantic state – swaddle firmly, pacifier and curl baby firmly against your body, gently clap infant on diapered bottom in a rhythmical manner, sway side to side, vertically rock, football hold, turn baby out from you, Hypersensitivity to stimuli – can include light, touch or loud noises. Closeness to people can make a baby frantic, even. Changes in muscle tone – the degree of stiffness in the baby’s muscles; either unusually limp or stiff or mixed tone. Because of tremors, jerking or other signs of distress the tensing of muscles is a sign of him trying to control uncomfortable sensations. Gastrointestinal problems – Wtery stools, diarrhea, excoriated buttocks, gas or constipation need attention. Stress and overstimulation in an infant can increase gastrointestinal distress.
Ways to support our caregivers • Respite!!! We all need breaks as parents and these can be difficult children to care for. • Teaching how to carefully monitor and read their infant and his signs or cues (one example of a program is on slide 24) • Working closely with medical staff to rule out any medical concerns that may mimic drug exposure symptoms • Education about positive expectations despite children’s drug exposure (the impact of environment is more important than the drug exposure alone)
Recommendations for those caring for the Alcohol and/or Drug Exposed Infant or Toddler • Establish routines • Understand normal behavior patterns for young children • Avoid over stimulation • Anticipate and prevent stressful situations • Infant Massage • Tummy time • Use developmentally appropriate toys to play with children • Repeated mental health screening • Repeated developmental-behavioral screening • Labeling children as “FASD”, “meth babies”, “crack babies”, etc. can harm them • Safe, loving, nurturing home
PIC’s PFR training • A 10-week program that focuses on children’s social emotional development based on research that says healthy infant development rests on the foundation of relationships — relationships that help babies feel secure and confident that their needs will be met as they explore their worlds. Extensive research has shown that the quality of experiences in the first 3 years of life has a profound impact on later development, including how children perform in school and their ability to form satisfying relationships with teachers, friends and others. Having caring relationships with sensitive parents or other primary caregivers is the most important factor in determining later outcomes • This is a research-based program developed by the University of Washington’s school of nursing • Our role is to give information on the social and emotional needs of young children and how caregivers can/are meeting those needs • Videotaping promotes reflective parenting (tuning into own and child’s feelings) • Caregiver’s role is to feel empowered and supported to use the information and strategies in their interactions with children
Behnke, M. & Smith, V.C. Prenatal Substance Abuse: Short- and Long-term Effects on the Exposed Fetus. Pediatrics; http://pediatrics/aappublications.org/content/early/2013/o2/20/peds.2012-3931 Davies & Bledsoe, Prenatal alcohol & drug exposures in adoption. Pediatric Clinics of North America. 2005. Rosen TS, Johnson HL. Long-term effects of prenatal methadone maintenance. NIDA Res Monogr 1985; 59: 73-83. Lester BM, Arria AM, Derauf C, Grant P, LaGasse L, Newman E, Shah RZ, Stewart S, & Wouldes T. Methamphetamine Exposure: A Rural Early Intervention Challenge National Abandoned Infants Assistance Resource Center: Fact Sheet on Prenatal Substance Exposure. UC Berkeley. (March 2012). http://aia.berkeley.edu References:
Resources • Early Support for Infants and Toddlers (ESIT, or “birth to 3 program”) provides early intervention services, including family resources coordination, for eligible children from birth to age 3 and their families. Family Resources Coordinators (FRCs) are in each county or geographic area of the state. They can help a family access early intervention services a child may need. A family can also call their local health department or school district or a health care provider about their concerns. They can provide a screening or suggest other resources. • Providence Children’s Center (425) 258-7311 (ESIT, PIC program, or general evaluations for children of all ages) • Fetal Alcohol Syndrome Diagnostic Clinic, Everett (425) 258-7444 • http://www.adoptmed.org • http://depts.washington.edu/fasdpn • http://www.nofas.org • Seattle Children’s hospital and regional medical center 206-987-2000, 866-987-2000 (toll-free) • http://www.zerotothree.org • http://www.cdc.gov • http://aia.berkeley.edu • http://Pediatrics.aapublications.org