Download
1 / 45
470 likes | 528 Views
Learn about the processes of tubular reabsorption and secretion in nephrons, mechanisms of transport, and key factors influencing urine formation in the renal system. Explore the intricate roles of active and passive transport, osmosis, and hormonal control in maintaining fluid and electrolyte balance.

E N D
Tubular reabsorption & Secretion Dr. Eman El Eter
Introduction • Urinary excretion = Glomerular Filtration –Tubular reabsorption + Tubular secretion. Tubular secretion means: the net movement of solutes from peritubular capillaries into the tubules.
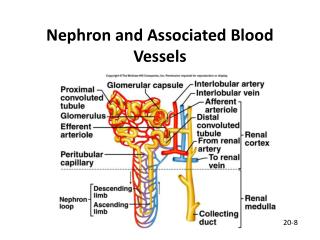
What are the routes through which a substance enter the tubules? 1- Glomerular filtration. 2- Secretion from the peritubular capillaries which occurs in two steps: a. simple diffusion of the substance from peritubular capillaries into renal inerstitium. b. movement across the tubular epithelium into the lumen through active or passive transport.
Mechanisms of tubular transport: • Active transport: • Primary active transport: e.g. Na-K-pump, H+-pump • Secondary active transport : e.g. Na-K-2Cl co-transport, glucose-sodium co-transport, amino acid-sodium co-transport. • Passive transport: • Simple diffusion e.g. Cl, HCO3-, urea. • Facilitated diffusion glucose at the basal border. • Osmosis. • Thus the molecules moves through ion channels, transporters, pumps & exchangers. • Pinocytosis/ exocytosis.
Primary Active transport Examples: • Sodium potassium ATPase, • Hydrogen ATPase, • Hydrogen potassium ATPase, and • Calcium ATPase. Carrier, direct source of Energy ATP, against electrochemical gradient High conc Na transport through PCT
Secondary active transport • One of the substances (e.g., sodium) diffuses down its electrochemical gradient,the energy released is used to drive another substance (e.g. glucose) against its electrochemical gradient. Both bind to one carrier protein to be transported together. • Thus, secondary active transport does not require energy directly from ATP. • The direct source of the energy is that liberated by the simultaneous facilitated diffusion of another transported substance down its own electrochemical gradient. • The electrochemical gradient for Na is maintained by Na/K pump..
Secondary active transport, cont…… • Na-K-2Cl transport • In thick ascending limb of Henle • “loop” diuretics as furosemide, inhibits the action of the sodium 2-chloride, potassium cotransporter.
Simple diffusion Reabsorption of Chloride, Urea, and Other Solutes by Passive Diffusion Negative ions such as chloride are transported along with sodium because of electrical potentials. Urea: Inner modulary collecting duct, passive urea reabsorption is facilitated by specific urea transporters
Osmosis • Transport of solutes out of the tubules by either primary or secondary active transport, makes their concentration inside the cells to decrease while increase in the renal interstitium. This creates a concentration difference that causes osmosis of water in the same direction that the solutes are transported, from the tubular lumen to the renal interstitium. • Water reabsorption is mainly coupled to sodium. • Permeability differs through the nephron. • Route: Paracellular via tight junctions • Effect of ADH (Distal & collecting tubules).
Transport through PCT • Criteria of PCT: • Highly metabolic cells, rich in mitochondria. • Transporter proteins & channels. • Wide surface area of brush border, basolateral membrane
Renal tubular reabsorption through PCT • Solute reaborption in the proximal tubule is isosmotic (water follows solute somatically and tubular fluid osmolality remains similar to that of plasma= equal amount of solute and water are reabsorbed). • 65%-70% of water and sodiumreabsorption occurs in the proximal tubule • 90% of bicarbonate, calcium, K+ • 100% of glucose & amino acids. • Secretion: organic acids and bases such as bile salts, oxalate, urate, and catecholamines, certain drugs, such as penicillin and salicylates, • Proximal tubules: coarse adjustment. • Distal tubules: fine adjustment (hormonal control).
Loop of Henle • Responsible for producing a concentrated urine by forming a concentration gradient within the medulla of kidney. • When ADH is present, water is reabsorbed and urine is concentrated. • Counter-current multiplier.
Absorption through loop of Henle: • Descending limb: is water permeable and allow absorption of 25% of filtered H2O. It is impermeable to Na-CL. • Thin ascending limb: is impermeable to H2O, but permeable to Na-Cl, where they are absorbed passively in this part . • Thick ascending limb: is impermeable to H2O. Na-K-2Cl co-transport occur in this part. By the end of ascending limb of loop, the tubular fluid becomes hypo-osmolar to plasma.
Distal convoluted tubule and collecting ducts • What happens here depends on hormonal control: • Aldosterone affects Na+ and K+ • ADH – facultative water reabsorption • Parathyroid hormone – increases Ca++ reabsorption. • Fine adjustment of tubular filtrate takes place here according to body needs. • The first portion of DCT forms part of JGA, that provides feedback control of GFR and RBF of the same nephron. • The next early portion has the same characteristics as ascending limb of Henle that is impermeable to water but absorbs solutes. So it is called the diluting segment & the osmotic pressure of the fluid ~ 100 mOsm/L.
Late distal tubule& collecting tubules • Have similar functional characteristics. • Composed of two types of cells: • a. Principal cells: absorb Na+& H2O and secrete K+ • b. Intercalated cells: absorb K+ & secrete H+ • Impermeable to Urea. • water permeability under ADH • Secretion of K+ and reabsorption of Na+ controlled by aldosterone.
Medullary collecting ducts • Reabsorb <10% of sodium & H2O. • Final site for processing urine and so determine final urine output of H2O & solutes • Characteristics: - Under ADH control. -Highly permeable to urea. -Secretes H+ against conc gradient (role in acid-base balance).
Na+, K+, H+ urea
Distal convoluted tubule and collecting ducts • Tubular secretion to get rid of substances: K+, H+, urea, ammonia, creatinine and certain drugs • Secretion of H+ helps maintain blood pH (can also reabsorb bicarb and generate new bicarb)
Na+ absorption • Na & Cl reabsorption plays a major role in body electrolyte and water metabolism. • Na+ transport is also coupled to the movement of H+, K+, glucose, amino acids. • Na+ absorption occurs by many mechanisms depending on the part of nephron: • 1- active transport mechanism: • E.g. Collecting tubules & ducts. • 2- Passive at the thin ascending limb • 3- Co-transport: thick ascending • i.e. Active all through except thin ascending limb.
From tubular lumen into tubular cells Na+ moves by; Exchanger Co-transport. It helps reabsorption of nutrients Na+ is pumped into the interstitium by Na+-K+ ATPAse
Glucose handling • Glucose absorption also relies upon the Na+ gradient. It is absorbed by Na-glucose co-transport. • Most reabsorbed in proximal tubule. • At apical membrane, needs Na+/glucose cotransporter (SGLT) • Crosses basolateral membrane via glucose transporters (GLUT’s), which do not rely upon Na+.
Tubular transport maximum for glucose • Essentially all glucose is reabsorbed • Tmg = 375 mg/min in men and 300 mg/min in women. • The renal threshold for glucose= 180 mg/dl • Handling of glucose is limited by saturation of the transport mechanism i.e. carriers.
Glucose titration curve • Ideal curve occurs if Tmg in all tubules is identical and if glucose was removed from all tubules . • Actual curve is rounded (dashed line) and deviates from the ideal curve. This deviation is called splay. • The magnitude of the splay is inversely proportionate to the avidity with which the transport mechanism binds the substance it transports.
Water reabsorption • PCT: 65% of filtered water reabsorbed. • Descending loop of Henle:20-25% . • Ascending limb= zero water reabsorbed. • Distal tubules & collecting tubules: under ADH control
Regulation of tubular reabsorption • There must be a balance between tubular reapsorption and glomerular filtration. • This is controlled by local , nervous & hormonal mechanisms. • Do you think that water and solutes are dependently regulated? • 1.Glomerulotubular balance; prevents overloading of distal parts when GFR increases. • 2. Peritubular capillary reabsorption is regulated by hydrostatic and colloidal pressures through the capillaries. • 3. ABP: if increased it reduces tubular reapsorption: autoregulation.
Regulation of tubular reabsorption, cont…… • 4-Tubuloglomerular feedback: • What is its physiological importance?
Regulation of tubular reabsorption, cont…… • 4. Hormonal: • - Aldosterone: Na+ Reabsorption, K+&H+ secretion • -Ang II.: (+)Aldosterone • ADH (+) H2O2 reabsorption • ANP: (+)Na+ excretion & diuresis • Parathyroid hormone: Increases calcium reabsorption & decreases phosphate reabsorption. • Nervous: Sympathetic: -Increases Na+ reabsorption.
Secondary active secretion This transport is mediated by a specific protein in the brush border of the luminal membrane. • As sodium is carried to the interior of the cell, hydrogen ions are forced outward in the opposite direction into the tubular lumen. • The Na+ electrochemical gradient is utilized by the exchanger to extrude H+ from the cell with a 1 Na+ : 1 H+ coupling; Na+-H+ counter transport Proximal tubules
K+ handling • K+ is the major cation in cells and its balance is essential for life. • Small change from 4 to 5.5 mmoles/L = hyperkalaemia • K+ is reabsorbed at proximal tubule. • Changes in K+ excretion due to changes in K+secretion in distal tubule
K+ handling • K+reabsorption along the proximal tubule is largely passive and follows the movement of Na+ and fluid. • K+secretion occurs in cortical collecting tubule (principal cells), and relies upon active transport across basolateral membrane and passive exit across apical membrane into tubular fluid.