Download
1 / 16
160 likes | 404 Views
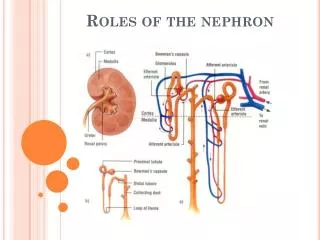
Reabsorption and the Nephron 3/19 and 3/21 . How does solvent drag pull water out of the filtrate through transcellular and paracellular routes? How does solvent drag explain the diuresis associated with diabetes? What is the function of the Loop of Henle?

E N D
Reabsorption and the Nephron 3/19 and 3/21 • How does solvent drag pull water out of the filtrate through transcellular and paracellular routes? • How does solvent drag explain the diuresis associated with diabetes? • What is the function of the Loop of Henle? • How does the Loop function as a Counter Current Multiplier? • What is the function of the Distal Convoluted Tubule? • What is the function of the Collecting Duct? • How does the collecting duct help control the pH of your blood with our beloved enzyme carbonic anhydrase? • Why is it impossible to modify urine quality after it leaves the collecting duct? • What happens when glucose remains in the urine?
Polar Molecules, such as glucose or sodium, carry spheres of hydration with them when they are reabsorbed into the blood or are “NOT” reabsorbed and remain in the urine causing diuresis.
The Proximal Convoluted Tubule (PCT) is the ONLY place in the nephron that can reabsorb glucose from the filtrate. Why might the urine taste “sweet” if your diabetes mellitus is uncontrolled? Why might DM cause diuresis (large amounts of urine)? • Na+ and Glucose are co-transported by enzymes have a transport maximum- • Only so many glucose molecules can be removed from the filtrate/minute (Tmax). • Glucose freely filtered from the blood- • Only PCT can reabsorb glucose- • Glucose has a sphere of hydration- • IF the Tmax passed: glucose stays in urine forever- • Each glucose that stays in urine carries water with it! • OligouriaDehydrationWhy are you so thirsty? • What will posterior Pituitary try to do with ADH? • What will adrenal cortex try to do with aldosterone? • Diabetes mellitus-VS.-Diabetes insipidus-
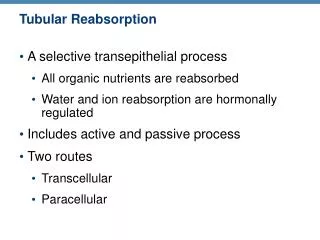
Concentration gradients and semipermeable membranes: If there is more of a polar molecule on one side of a membrane than the on other, several things could occur. The polar molecule (solute) could pass through until both sides have equal solute concentrations. If polar molecules pass through, they may carry water hydrogen bonded to them If polar molecules pass through, they may attract water when they get to the other side. If the pores of the membrane are too small and do not allow the solute to pass, they MAY allow the solute to diffuse via transcellular or paracellular pathways.
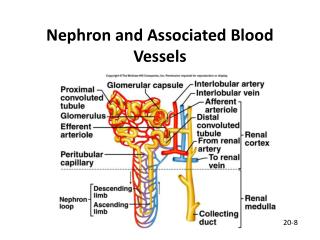
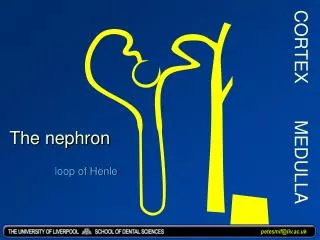
LOOP OF HENLE IS AN AMAZING COUNTER CURRENT MULTIPLIER FOR SALTS AND UREA. (180 L about 35L)(Extra credit: figure it out in class you get a Nobel Prize and a “A” for AP212 ) • Loop reabsorbs 15-20% of water: fine tuning of water reabsorption only occurs if salts pumped out of ascending loop! • Ascending Loop (THICK): water impermeable. Na/K ATPase moves intracellular Na+ into interstitium, so Na+ is pulled into cell from filtrate along with K+ and 2 Cl- ions by a Na+K+-2Cl- pump. • Descending Loop (THIN): Very permeable to water and salts • Idea #1: Salts are pumped into the interstitium from the thick Ascending Loop that drag H2O out of permeable thin Descending Loop • Idea #2: Reabsorbed water passes into the capillaries of the vasa recta out before water can diffuse back into the filtrate (whisk away). • Idea #3: Concentration gradient along Loop established by a Counter Current Mechanism along length of Loop. • Idea #4: Cortical vs. Medullary Loops: degree of water reabsorption dependent on length of Loop. • Volume of filtrate is further decreased UREA ALSO appears to be critical for dragging water away from the filtrate! Concentration gradients established here help reabsorb water from collecting duct!
The Loop of Henle only works if the thick ascending side is pumping NaCl and KCl (very polar) out of the filtrate into the interstitium. This drags water out of the descending side (water attempts to dilute the salts)! Water is dragged into the protein-rich plasma vasa recta (protein acts like sponge) and the reabsorbed water is whisked away.
The longer the Loop of Henle, the greater the osmotic gradient and the greater amount of water you can remove from the descending loop AND collecting duct! Note that urea is being pumped out and recirculated in the Loop, urea helps draw extra water out of the collecting duct “if the CD is H2O permeable” and if the interstitium is hyperosmotic (“salty”).
Short Loop: Long Loop: Counter Current Multipliers: Why do short “cortical” loops produce dilute urine? Why are long “medullary” loops best at producing concentrated urine? Remember that the gradient established by the ascending loop can also pull water from the lumen of the collecting duct.
Why is reabsorbed fluid “whisked” away from the tissues around the nephron or collecting duct? • Hydrostatic pressure in capillary= +15 mmHg out of capillary • Remember the blood entering this capillary was filtered in the glomerulus! • Hydrostatic pressure in FILTRATE= -5 mmHg out of capillary • Remember: pressure gradient is required to drive filtrate towards the bladder! • Osmotic pressure in plasma= -28 mmHg into capillary • Remember: the number of proteins in this blood has not changed! • Osmotic pressure in filtrate= 0 mmHg essentially zero! • Hopefully NO protein was filtered! • Net Filtration Pressure: • (+15 out)+(-5 in) + (-28 in) + (0) = +15 -33 = -18 mmHg INTO capillary! • Therefore fluid in the interstitium wants to enter the blood in the capillary! • Remember! The nephron or collecting duct must be made “permeable” to water for this to occur!
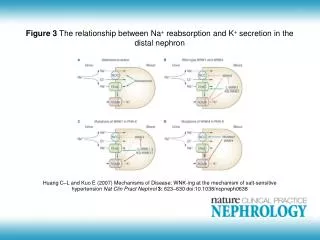
DISTAL CONVOLUTED TUBULE CAN REABSORB ABOUT 10% OF THE FILTRATE AND ACTIVITY IS HORMONE DEPENDENT. When the filtrate enters the DCT it is not too different from the plasma in terms of osmolarity! Aldosterone acts on the DCT (and collecting duct) and activates the Na+/K+-ATPase and causes active reabsorption of Na+ out of the filtrate Na+/K+-ATPase trades 3Na+ from filtrate for 2 K+, this conserves Na+ in the body at the cost of K+! Because sodium has a LARGE sphere of hydration and because potassium has a SMALL sphere of hydration, water is conserved if sodium is conserved (reabsorbed). V.I.P.! If sodium is not removed from the filtrate in the DCT, then less water is removed from DCT. Aldosterone Absence: ↑body loss of Na+, ↑urine Na+, ↑urine volume. • DCT is also important for calcium reabsorption, a hormonal effect related to increased plasma parathyroid hormone and calcitriol. • Finer tuning of H+ balance in body also begins here.
COLLECTING DUCTS PROVIDE THE LAST PLACE FOR THE FINE TUNING URINE VOLUME, pH, AND SALT BALANCE. URINE CONTENT IS FINE TUNED BY TWO C.D. CELL TYPES. Principle Cells: reabsorb Na+ and secrete K+ into urine (Na/K-ATPase) 3Na+from cell move into interstitium and 2K+ from interstitium move into cell SO…. Na+ passively diffuses into cell from lumen in exchange for K+ Water follows sodium and is thus conserved at the cost of potassium loss Intercalated Cells: several options to prevent acidosis in blood! Direct Proton Secretion: H+-ATPase direct pumping into lumen causing the blood pH to become less acidic, urine becomes more acidic. Proton Trading (Indirect H+ removal): Na+ or K+ in lumen exchanged for H+ in cell, as a result blood has fewer H+ and urine becomes acidic (Aldosterone Dependent). Anytime H+ appears in the urine, the urine volume may increase (potential for dehydration).
The Importance of Aquaporin • The Importance of ADH (Vaspresssin) from the posterior pituitary. • Hormone ADH moves Aquaporin to plasma membrane. • ADH causes the collecting duct to be permeable to water!
Golden Rule: If you want to lose something, filter it then don’t reabsorb it, just remove water and concentrate the leftovers. You can “filter” or “secrete” protons into filtrate to remove them!A similar processes occur in the PCT and collecting duct Intercalated Cells of CD Acetazolamide (Diamox) is a drug that is filtered and blocks carbonic anhydrase, what will happened to urine/blood pH?
THE DISTAL CONVOLUTED TUBULE AND COLLECTING DUCTS HAVE THREE DIFFERENT WAYS TO FINE TUNE OR “BUFFER” CHANGES IN BLOOD pH (prevent acidosis of blood). • 1) Secondary Active exchange in the PCT: • Interstitial Cl- exchanged for intracellular HCO3- • Keep the base, lose the acid • 2) Aldosterone can move a H+/Na+-exchanger to the plasma membrane of collecting duct cells -Dump H+/Save Na+ • 3) Na/K-independent H+-ATPase in Collecting Duct • Directly pump protons into lumen • Chloride ions chase after H+ in the filtrate for electrical neutrality. H+-ATPase pumps up to a X1,000 gradient • Urine pH limit is a pH of about 4.5 (about like vinegar). • This is the absolute limit of our pH compensation. If you can’t compensate for changes in blood pH after all these H+ secretion mechanisms are at maximal activity? Hello Comma!
Collecting Duct is the last chance to fine-tune the quality of the urine. • Once urine leaves CD where does it go? • Urine enters the minor calyxmajor calyxureterbladder • Urine exits body when smooth muscle of bladder contracts and urine is forced out the urethra. • Once urine leaves CD its qualities cannot be altered! • There are no pumps of pathways to alter the quality of the urine after it leaves the collecting duct!
WHY WAS THE TASTE OF SUGAR IN THE URINE ONE OF THE FIRST BIOCHEMICAL TESTS FOR DIABETES DIAGNOSIS? • Enzymes have a transport maximum- • Glucose freely filtered from the blood- • Only PCT can reabsorb glucose- • Glucose has a sphere of hydration- • Tmax passed: glucose stays in urine- • Polyuria (large urine volume) >> Dehydration >>>>> • Diabetes Mellitus (sweet taste)- Insulin Problem • VS. • Diabetes Insipidus (no sweet taste)- ADH Problem • Why can a large urine volume rapidly become FATAL?