Download
1 / 20
210 likes | 549 Views
Abdominal Wall Defects. Priscilla Joe, MD Children’s Hospital and Research Center at Oakland. Omphalocele. Membrane sac arising from the umbilical cord covers intestines Outer membrane layer consists of amnion and inner lining of peritoneum

E N D
Abdominal Wall Defects Priscilla Joe, MD Children’s Hospital and Research Center at Oakland
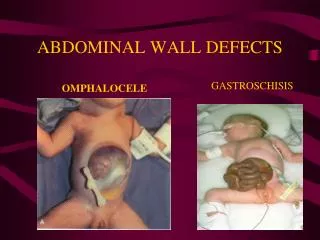
Omphalocele • Membrane sac arising from the umbilical cord covers intestines • Outer membrane layer consists of amnion and inner lining of peritoneum • Size ranging from small->giant defects containing liver, small and large bowel, stomach, spleen, ovaries, and testes • Associated with foreshortened bowel and malrotation • Small abdominal cavity and pulmonary hypoplasia
Gastroschisis • No membrane covering • Abdominal wall defect typically 2-4cm diameter • Lateral to the right side of the umbilical cord • Usually contains midgut and stomach • Thickened, atretic, and possibly ischemic bowel • Associated with malrotation
Embryology of Gastroschisis • Failure of vascularization of the abdominal wall due to abnormal involution of the right umbilical vein or a vascular accident of omphalomesenteric artery causes abdominal wall weakness and subsequent rupture • Rupture of a small omphalocele with absorption of the sac and growth of a skin bridge between the abdominal wall defect and umbilical cord
Embryology of Omphalocele • Normally, midgut returns to the abdomen by 10th week of gestation • Somatic layers of cephalic, caudal, and lateral folds join to close abdominal wall • With omphalocele, folds fail to close
Gastroschisis and Omphalocele • Combined incidence of 1 in 2000 births • Male-to-female ratio is 1.5:1 • Overall survival > 90%
Gastroschisis • Increasing incidence • Associated with young maternal age and low gravida • Associated with prematurity and low birth weights
Omphalocele • Incidence has remained constant • Increased risk with advanced maternal age • Probable genetic predisposition • Associated syndromes and anomalies (45-55%): - gastrointestinal - cardiac - trisomy 13, 18, 21 - OEIS complex (omphalocele, bladder extrophy, imperforate anus, spinal defects - Beckwith-Wiedemann - pentalogy of Cantrell - cleft palate - pulmonary hypoplasia • May be associated with maternal use of valproic acid
Diagnosis • AFP synthesized in fetal liver and excreted by fetal kidneys and crosses placenta by 12 weeks • Elevated maternal MSAFP in neural tube defects, abdominal wall defects, duodenal or esophageal atresia • 40% false positive rate • Fetal ultrasound after 14 weeks gestation • Amniocentesis and fetal echocardiography
Treatment • NGT to low intermittent suction • Use of bowel bags, saran wrap • Conservation of body heat and fluid losses • Antibiotics • Careful positioning to avoid kinking of mesenteric vessels • 1.5 times maintenance fluids with isotonic fluids
Surgical Management • Operative repair within 2-4 hours of birth • Primary closure for smaller defects • Delayed primary closure for large defects • Avoid compromised ventilation and abdominal compartment syndrome • Use of silo with sequential reduction of abdominal contents • Later fascial closure
Mortality/Morbidity • Short gut syndrome • NEC • Gut dysmotility and prolonged ileus • Sepsis • Complications from associated anomalies/syndromes