Download
1 / 16
550 likes | 2.47k Views
GASTROSCHISIS. ABDOMINAL WALL DEFECTS. OMPHALOCELE. Exomphalos and gastroschisis are two different congenital anomalies Overall incidence is approximately 1: 3000 live births Usually diagnosed prenatally on ultrasound Exomphalos and gastroschisis can usually be differentiated prenatally

E N D
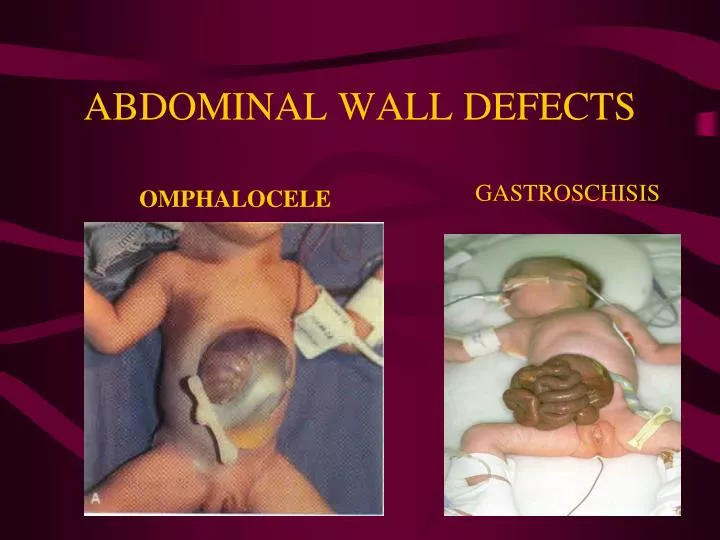
GASTROSCHISIS ABDOMINAL WALL DEFECTS OMPHALOCELE
Exomphalos and gastroschisis are two different congenital anomalies Overall incidence is approximately 1: 3000 live births Usually diagnosed prenatally on ultrasound Exomphalos and gastroschisis can usually be differentiated prenatally Do not inevitably require delivery by caesarian section Differ markedly in their clinical appearance
Exomphalos (omphalocele) • CONGENITAL Anterior abdominal wall defect at the base of the umbilical cord with herniation of the abdominal contents
Pathophysiology • Failure of the midgut to return to abdomen by the 10th week of gestation
Clinical Findings • central defect of the abdominal wall beneath the umbilical ring. • Defect may vary from 2-10 cm • Always covered by sac • The sac may be intact or ruptured • Sac is composed of amnion, Wharton’s jelly and peritoneum • The umbilical cord inserts directly into the sac in an apical or occasionally lateral position. • Sac contains intestinal loops, liver, spleen and bladder , testes/ovary • >50% have associated defects • Prognosis depends on theses associated anomalies • Mortality is approximately 40%
GASTROSCHISIS • Congenital defect of the anterior abdominal wall just lateral to the umbilicus
Pathophysiology • Rapid dissolution of the right umbilical vein after the standard period of organogenesis leaves an area of relative weakness in the mesenchyme through which bowel or abdominal viscera can herniate and eventually rupture. • Rupture of a small omphalocoele
Clinical Findings • Defect to the right of an intact umbilical cord allowing extrusion of abdominal content • Umbilical cord arises from normal place in abdominal wall • Opening 5 cm • No covering sac (never has a sac ) • Evisceration usually only contains intestinal loops • Bowels often thickened, matted and edematous • Infants have better prognosis than those with an omphalocele (Mortality is approximately 10% ) • 10-15% have associated anomalies (intestinal atresia) • 40% are premature/SGA
MANAGEMENT • ABC • Heat Management • Sterile wrap or sterile bowel bag • Radiant warmer • Fluid Management • IV bolus 20 ml/kg RL/NS • D10¼NS 2 maintenance rate • Nutrition • NPO and TPN • Gastric Distention • OG/NG tube • Infection Control • Ampicillin and Gentamicin • Associated Defects • Closure of the defect (see next slides)
Omphalocele • Conservative treatment • Reduction by squeezing the sac or placement of a silo for sequential tightening and staged closure • Children with giant omphaloceles or concomitant problems that make them poor anesthetic risks may be treated with topical application of Betadine ointment or silver sulfadiazine to the intact sac. This allows secondary eschar formation and eventual epidermal ingrowth. Residual abdominal wall hernias are then repaired at 1 year of age. • Surgical treatment • Primary closure • Staged closure
Gastroschisis • Often be treated by direct full-layer closure of abdominal wall • May be associated with postoperative gut dysfunction Usually require postoperative nutritional and ventilatory support
UMBILICAL HERNIA • all pediatric umbilical hernias are congenital and form as a hernia through a persistent umbilical ring. • subcutaneous tissue and skin covering the protruding bowel • Incidence : one in every six live birth • Premature and low birth weight infants have a higher incidence than full-term infants • spontaneous resolution rates of 83% to 95% by 6 years of age, so it seems very safe to simply observe the hernia to allow closure to occur. • If complications occur, the defect is large or defect not close spontaneously surgical closure is indicated
EPIGASTRIC HERNIA • Hernias of the abdominal wall through the midline linea alba, termed epigastric hernias, • Presents as small masses, between the umbilicus and xiphoid process. • usually contains extra peritoneal fat. • Can be multiple. • Epigastric hernias do not resolve and should be repaired.