Download
1 / 70
710 likes | 763 Views
Explore the intricate pathways of purine metabolism, encompassing de novo synthesis, salvage pathways, biosynthesis of purine nucleotides, and catabolism in the body. Learn about key enzymes, reactions, and regulation of purine nucleotide synthesis while delving into disorders like gout and Lesch-Nyhan syndrome.

E N D
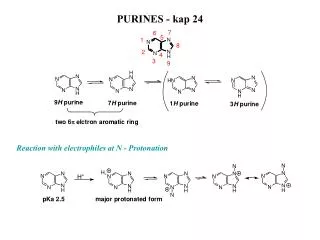
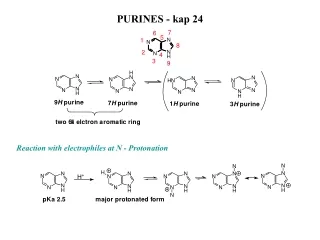
METABOLISM OF PURINES
NH2 N O N N HN N N H H2N N H N PURINES Guanine Adenine
PYRIMIDINES O CH3 NH2 HN 4 O 3N 5 6 o N H 2 HN o N H o N H Thymine Cytosine Uracil
+ Phosphate Nitrogenous Base + Sugar • Nucleoside • Nucleotide
DIGESTION OF NUCLEIC ACIDS Ribonuclease Nucleic acids Nucleotides Deoxyribonuclease Nucleosides + PO42- Nucleotides Nucleotidases free bases+ pentose sugar Nucleosides Nucleosidases
BIOSYNTHESIS OF PURINE NUCLEOTIDES • Liver is the major site. • Two pathways: 1. De novo synthesis 2. Salvage pathway • Operates in the Cytoplasm
DE NOVO SYNTHESIS • Purine ring synthesis from different small components (amphibolic intermediates)
N 7 8 C 9 N C 6 N 5 1 C 4 C C 2 3 N Sources of carbon and nitrogen in the purine ring CO2 GLYCINE ASPARTATE N5 N10methenyl TETRAHYDROFO LATE N10FORMYL TETRAHYDROFOLATE GLUTAMINE GLUTAMINE
Reactions HMP Shunt Pathway PHOSPHORIBOSYL PYROPHOSPATE (PRPP) PRPP SYNTHASE D-RIBOSE 5’ P ATP AMP GLUTAMINE PRPP GLUTAMYL AMIDOTRANSFERASE GLUTAMATE Amino acids 5’ PHOSPHORIBOSYL AMINE (PRA) FH4 CO2 IMP GMP AMP
Synthesis of Nucleoside triphosphates (NTP’s) • Nucleoside monophosphate(GMP, AMP) ATP KINASE ADP • Nucleoside diphosphate(GDP,ADP) ATP KINASE ADP • Nucleoside triphosphate(GTP, ATP)
SALVAGE PATHWAY: . • Phosphoribosylation of purines and Phosphorylation of purine nucleosides • Recycling of purines formed by degradation of nucleotides. • Enzymes: APRTase, HGPRTase andkinases • Important in RBCs and brain • Less energy consumption
SALVAGE PATHWAY: . 1. Salvage Reactions by phosphoribosylation of purine bases • 2. Salvage Reactions by phosphorylation of purine nucleosides
1. Salvage Reactions by phosphoribosylation of purine bases Adenine -Adenine phosphoribosyltransferase Hypoxanthine Hypoxanthine –guanine phosphoribosyltransferase Guanine
1. Salvage Reactions by phosphoribosylation of Adenine ADENINE PHOSPHORIBOSYL TRANSFERASE AMP Adenine PRPP PPi
1. Salvage Reactions by phosphoribosylationof Hypoxanthine HYPOXANTHINE –GUANINE PHOSPHORIBOSYLTRANSFERASE IMP Hypoxanthine PRPP PPi
1. Salvage Reactions by phosphoribosylation of Guanine HYPOXANTHINE –GUANINE PHOSPHORIBOSYL TRANSFERASE GMP Guanine PRPP PPi
2. Salvage Reactions by phosphorylation of purine nucleosides GUANOSINE KINASE GMP Guanosine ATP ADP Adenosine ADENOSINE KINASE • AMP ATP ADP
Regulation of Purine nucleotide synthesis • PRPP pool size • - ribose 5-phsophate and PRPP synthase. • PRPP glutamylamidotransferse • Hypoxanthine guanine phosphoribosyltransferase
Ribose 5-phosphate + ATP • PRPP • ( ) • 5-Phosphoribosylamine • IMP AMP GMP ATP GTP
CATABOLISM OF PURINES H2O NH3 IMP AMP GMP AMP DEAMINASE H2O H2O Pi 5’ NUCLEOTIDASE Pi ADENOSINE 5’ NUCLEOTIDASE Pi GUANOSINE H2O RIBOSE-1 P H2O ADENOSINE DEAMINASE PURINE NUCLEOSIDE PHOSPHORYLASE NH3 Pi INOSINE GUANINE PURINE NUCLEOSIDE PHOSPHORYLASE Pi H2O GUANASE O2+H2O RIBOSE-1-P NH3 XANTHINE HYPOXANTHINE XANTHINE OXIDASE O2+H2O XANTHINE OXIDASE H2O2- H2O2- URIC ACID
URIC ACID • Total body urate pool : 800 to1600 mg in ♂ 500 to 700 mg in ♀ • Turnover rate : 600 mg / 24hrs . • Normal uric acid level : 2 - 5 mg / dL in ♀ 3 - 7 mg / dL in ♂
DISORDERS OF PURINE METABOLISM • Gout • Lesch – Nyhan syndrome Hyperuricemia Hypouricemia • Immunodeficiency(Adenosine deaminase deficiency)
GOUT Uric acid level > 7 mg / dl in males and > 6 mg / dl in females Hyperuricemia • Metabolic disease associated with hyperuricemia
GOUT • Types • Primary gout • Secondary gout
PRIMARY GOUT • Glucose-6-phosphatase deficiency. • Increased activity of Glutathione reductase • Abnormality in PRPP synthase. • Abnormality in PRPP Glutamylamidotransferase • Deficiency of enzymes of salvage pathway
Glucose 6 phosphatase Glucose Glucose 6 phosphate Glycogen GSH NADP HMP Shunt Pathway Glutathione reductase GSSG NADPH D-ribose 5’ P PRPP synthase PhosphoribosylPyrophospate (PRPP) PRPP glutamylamidotransferase 5’ Phosphoribosyl amine (PRA) HGPRTase Hypoxanthine IMP HGPRTase AMP GMP Guanine Hypoxanthine Uric acid
Glucose 6 phosphatase Glucose Glucose 6 phosphate Glycogen HMP Shunt Pathway D-ribose 5’ P PhosphoribosylPyrophospate (PRPP) 5’ Phosphoribosyl amine (PRA) IMP AMP GMP Hypoxanthine Uric acid
Glucose 6 phosphate Glycogen GSH NADP HMP Shunt Pathway Glutathione reductase GSSG NADPH D-ribose 5’ P PhosphoribosylPyrophospate (PRPP) 5’ Phosphoribosyl amine (PRA) IMP AMP GMP Hypoxanthine Uric acid
Glucose 6 phosphate Glycogen HMP Shunt Pathway D-ribose 5’ P PRPP synthase PhosphoribosylPyrophospate (PRPP) PRPP glutamylamidotransferase 5’ Phosphoribosyl amine (PRA) IMP AMP GMP Hypoxanthine Uric acid
HGPRTase HGPRTase Hypoxanthine IMP GMP Guanine Uric acid
HGPRTase HGPRTase Hypoxanthine IMP GMP Guanine
Glucose 6 phosphate D-ribose 5’ P PhosphoribosylPyrophospate (PRPP) 5’ Phosphoribosyl amine (PRA) HGPRTase Hypoxanthine IMP Uric acid
Glucose 6 phosphatase Glucose Glucose 6 phosphate Glycogen GSH NADP HMP Shunt Pathway Glutathione reductase GSSG NADPH D-ribose 5’ P PRPP synthase PhosphoribosylPyrophospate (PRPP) PRPP glutamylamidotransferase 5’ Phosphoribosyl amine (PRA) HGPRTase Hypoxanthine IMP HGPRTase AMP GMP Guanine Hypoxanthine Uric acid
SECONDARY GOUT • Increased turnover rate of nucleic acids. - Leukemias, polycythemia. - Treatment of Malignant tumors. - Psoriasis. • Reduced excretion rate. - Renal failure. - Thiazide diuretics. - Lactic acidosis and Ketoacidosis.
Clinical Manifestations • Pathophysiology • Accumulation of insoluble monosodium urate crystals • Kidneys • Joints
Clinical Manifestations • Clinical features 1. Acute arthritis – Accumulation in the synovial fluid leading to painful joints. Tophi (Deposition in cooler areas) Major joint involved-first meta-tarsophalyngeal joint
Clinical Manifestations • Clinical features 1. Acute arthritis Precipitating factors- Alcohol Alcohol • Lactic acidosis Decreases renal excretion of uric acid Increased serum uric acid levels 2. Renal lithiasis– Precipitation of insoluble sodium urate crystals in the kidneys and ureter leading to stone formation.
Treatment 1. Allopurinol 2. Probenecid 3. Restrict alcohol
1. Allopurinol Mechanism of action 1. By competitive inhibition • Allopurinol • (compeititive inhibitor) • Hypoxanthine • (Substrate) Allopurinol Nucleic acids Hypoxanthine Alloxanthine Xanthineoxidase Xanthineoxidase Xanthine Uric acid Gout
1. Allopurinol Mechanism of action 2. By suicide inhibition Nucleic acids Allopurinol Hypoxanthine Xanthine oxidase Xanthine oxidase Alloxanthine Xanthine Uric acid
2. Probenecid Mechanism of action Probenecid • Decreases the reabsorption of uric acid from renal tubules Increased renal excretion of uric acid Decreased serum uric acid levels 3 . Restrict alcohol
LESCH NYHAN SYNDROME • ‘ X linked ’ disorder of Purine metabolism. • Total or partial deficiency of HGPRTase • Features: - Self mutilation, mental retardation and ↑ uric acid. - Nephrolithiasis, gout.
HYPOURICEMIA • Adenosine deaminase deficiency. • Congenital xanthineoxidase deficiency • Purine nucleoside phosphorylase deficiency.
ADENOSINE DEAMINASE DEFICIENCY ATP AMP Ribonucleotide reductase ADENOSINE ADENOSINE DEAMINASE dATP INOSINE Prevent Formation of all d NTP HYPOXANTHINE XANTHINE Cells cannot make DNA URIC ACID
METABOLISM OF PYRIMIDINES
BIOSYNTHESIS OF PYRIMIDINE NUCLEOTIDES • Two pathways: 1. De novo synthesis 2. Salvage pathway • Subcellular site: Cytoplasm
DE NOVO SYNTHESIS • Pyrimidine ring synthesis from different small components (amphibolic intermediates) • PYRIMIDINE RING IS SYNTHESIZED BEFORE BEING • ATTACHED TO RIBOSE 5-PHOSPHATE ( DONATED BY • PRPP)