Download
1 / 87
980 likes | 1.51k Views
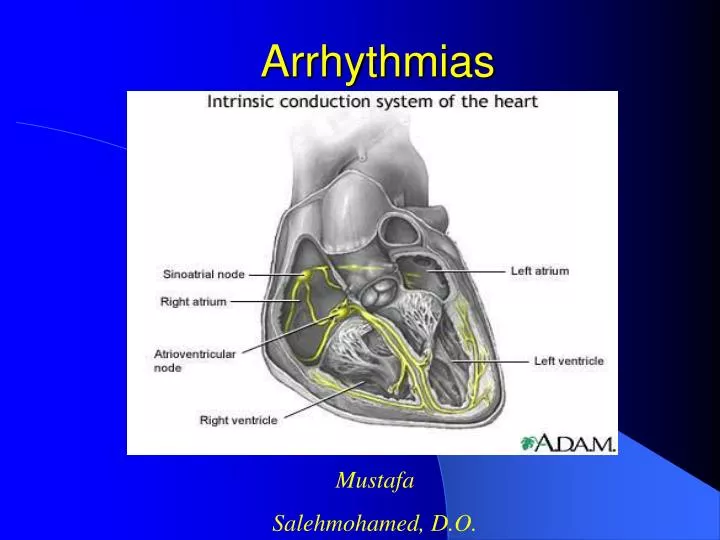
Arrhythmias. Mustafa Salehmohamed, D.O. DEFINITIONS. An arrhythmia is defined as any rhythm other than normal sinus rhythm Arrhythmias can be categorized as supraventricular or ventricular Supraventricular arrhythmias can be further divided into tachyarrhythmias or bradyarrhythmias.

E N D
Arrhythmias Mustafa Salehmohamed, D.O.
DEFINITIONS • An arrhythmia is defined as any rhythm other than normal sinus rhythm • Arrhythmias can be categorized as supraventricular or ventricular • Supraventricular arrhythmias can be further divided into tachyarrhythmias or bradyarrhythmias
SUPRAVENTRICULAR ARRHYTHMIAS
SUPRAVENTRICULAR ARRHYTHMIAS • Any arrhythmia arising above the bifurcation of the His bundle is classified as supraventricular. • The QRS complex morphology either can be normal or may be wide owing to bundle-branch or fascicular block (aberrant conduction) or conduction over an accessory pathway (anomalous conduction or pre-excitation). • Supraventricular cardiac arrhythmias can be further sub-categorized into tachyarrhythmias or bradyarrhythmias.
TACHYARRHYTHMIAS • Sinus tachycardia is defined as a rapid sinus rhythm with a HR > 100bpm • Tachyarrhythmia is defined as an arrhythmia with a HR > 100bpm • Supraventricular tachyarrhythmias can occur either as isolated premature complexes or in the form of nonsustained or sustained tachycardias
PREMATURE ATRIAL CONTRACTIONS • Premature atrial contractions (PACs) can arise from any part of the right or left atrium • The P wave morphology depends on the origin but differs from sinus rhythm • Frequent in normal persons and rarely cause symptoms • They are associated with respiratory disease, particularly in the presence of pulmonary hypertension
PREMATURE ATRIAL CONTRACTIONS • Other precipitating factors include coffee, tea, alcohol, sympathomimetic cold remedies • If an etiology cannot be determined and treatment is necessary, a Beta -blocker can be given
Atrial Flutter • Atrial flutter is much less common than Atrial Fibrillation (AF) • Its hemodynamic consequences and management are similar to that of AF • It is due to a large reentrant circuit (several centimeters) that involves the low lateral right atrium
Diagnosis • ECG shows flutter waves, which (depending on rate) may look like discrete P waves or merge to form a classic sawtooth pattern • The atrial rate is 250 to 350 beats/min The ventricular rate depends on the AV conduction but typically is 150 to 220 beats/min • QRS complexes usually are normal • Atrioventricular block may be consistent (2:1, 4:1, or rarely 3:1 or 5:1) or may vary
Signs and Symptoms • Symptoms depend principally on the resultant ventricular rate • If the rate is modest (< 120 beats/min) and regular (eg, stable 2:1 atrioventricular conduction), there may be no symptoms • Higher heart rates produce palpitations, and compromised cardiac output may produce dizziness and syncope
Treatment • Medical therapy more likely to slow down ventricular response than to restore NSR • Medications used : • Digoxin • Verapamil (works faster than digoxin but can cause hypotension • Beta-blockers • Class I drugs ( use with other drugs) • IV Ibutilide (risk of developing Torsades)
Treatment • If 1:1 conduction occurs with life-threatening rapid ventricular response rates (> 220 beats/min), immediate DC electroversion is indicated • Radiofrequency ablation (RFA) is emerging as an important approach for medically refractory atrial flutter. • The success rate is about 85% • Some patients develop AF after the procedure
Atrial Fibrillation • Atrial fibrillation (AF) is the most common sustained arrhythmia in adults • More than 2 million individuals in the United States have AF • With more than 160,000 new cases diagnosed every year • The incidence of AF increases with advancing age
Atrial fibrillation accounts for 1/3 of all patient discharges with arrhythmia as principal diagnosis. • 6% PSVT • 6% PVCs • 18% Unspecified • 4% Atrial Flutter • 9% SSS • 34% Atrial Fibrillation • 8% Conduction Disease • 10% VT • 3% SCD 2% VF Data source: Baily D. J Am Coll Cardiol. 1992;19(3):41A.
Prevalence of Atrial Fibrillation in the U.S. Estimated prevalence of atrial fibrillation in the United States.8
Etiology • Ischemic Heart Disease • Hypertensive Heart Disease • Rheumatic Valvular Disease • Cardiomyopathy • Non-rheumatic Valvular Disease • Congenital Hear Disease • CHF • Pericarditis • WPW
Etiology • Thyrotoxicosis • Pulmonary Embolism • Chronic Lung Disease • Pneumonia • Neoplastic disease • Post- operative states • Normal heart affected by: alcohol, stress, drugs, excessive caffeine, hypoxia, hypokalemia, hypoglycemia, infection
Atrial Fibrillation Morbidity and Mortality • Two fold increase in CV mortality • The most important consequence of AF are thrombo-embolic events and stroke • AF is one of the most potent risk factors for stroke • 4 – 6 fold increase risk of stroke/15 fold with h/o RHD • Persistent rapid ventricular rate associated with AF may lead to tachycardia induced cardiomyopathy (reversible) • Limitation in functional capacity from symptoms of palpitations, fatigue, dyspnea, angina, or CHF
Diagnosis • During AF, the atria have disorganized, rapid, irregular electrical activity exceeding 400 beats per minute • The ventricular response is also irregular and variable (irregularly irregular) • EKG: Absence of visible discreet P waves, or the presence of irregular fibrillation waves and an irregular ventricular response
Diagnosis • History – precipitating factors such as alcohol, caffeine, sympathomimetic drugs • Laboratory studies: Electrolytes, TFTs, substance abuse- toxicity screens • Echocardiogram • Holter (indicating arrhythmia: SVT, A. Flutter, Bradycardia induced) • EST ( R/O ischemia)
Signs and Symptoms • Palpitations • Chest Discomfort • Signs of CHF - 2° to loss of atrial kick or due to rapid rate • Weakness, faintness, and breathlessness • Symptoms and signs of systemic emboli (eg, stroke due to thrombus formation in the fibrillating atrium)
Atrial Fibrillation • Paroxysmal • Chronic (chronic paroxysmal) • Acute (onset within 24 – 48 hrs) • Lone (younger than 60, no HTN no CVD no Pulmonary disease)
Treatment • Treatment goals are management of any underlying (causative) disorder, control of the ventricular response rate, restoration of sinus rhythm, and prevention of emboli • Rate control vs. Rhythm control
Medications for Rate Control • Digoxin • Beta – blockers • Calcium channel blockers (diltiazem, verapimil) • Short-term control of ventricular rate in preparation for DC cardioversion is usually done with a beta -blocker or verapamil to avoid postconversion digoxin arrhythmias.
Cardioversion • Chemical Cardioversion • Class Ia and Ic Anti-arrhythmic Drugs (AEDs) • Amiodarone • in recent studies, prophylaxis with amiodarone before cardiac surgery has been found to decrease the occurrence of atrial fibrillation Aasbo, J et al.Amiodarone prophylaxis reduces major cardiovascular morbidity and length of stay after cardiac surgery: a meta analysis. Ann Intern Med 143: 2005.
Pharmacologic Cardioversion • Class Ia agents • procainamide (Procanbid) • quinidine (Quinidex, Quinaglute) • disopyramide (Norpace) • Class Ic agents • flecainide (Tambocor) • propafenone (Rhythmol) • Class III agents • amiodarone (Cordarone) - acute efficacy 16%-71% • sotalol (Betapace) • ibutilide - efficacy for flutter (63%), fib (31%) • dofetilide (Tikosyn)
Cardioversion • Electric cardioversion – method of choice for the hemodynamically compromised • Evaluate need for anticoagulation • R/O drug toxicity • Anesthesia • Synchronized 50 – 200 joules shock • Control of ventricular rate • AV nodal ablation with PPM • Pulmonary vein ablation (maintenance)
Atrial Fibrillation Management Rate control versus rhythm control • Advantage of maintaining NSR • Adverse effects of antiarrhythmics • After cardioversion even with antiarrhythmic therapy-50% develop recurrent A.F after cardioversion • Atrial Fibrillation Follow-up Investigation of Rhythm Management (AFFIRM) : Anticoagulation advantageous
AFFIRM • Atrial Fibrillation Follow-up Investigation of Rhythm Management • Hypothesis: Effect on mortality of antiarrhythmic therapy to maintain sinus rhythm vs. ventricular rate control alone, in the presence of anticoagulation • Primary endpoint: Total mortality • Secondary endpoint: Disabling CVA Cost of therapy Quality of life NHLBI AFFIRM Investigators. Am J Cardiol. 1997;79:1198-1202.
Atrial FibrillationManagement of the Risk of Stroke • 15 – 20% of ischemic strokes arise from emboli in the cardiac chambers and valves • AF accounts for 45% of embolic strokes • Majority of emboli arise in the LAA • Other sources of emboli: LV thrombus Mitral valve disease (including MVP and annular calcification), PFO Atrial septal aneurysm, and complex aortic atheromatous plaques • Cerebrovascular disease may also be a cause of stroke
Transesophageal Echocardiogram Showing Thrombus In this transesophageal echocardiogram, a thrombus (arrow) can be seen in the left atrial appendage (LAA).
Echocardiogram of Fibrillating Left Atrium The smokelike echoes, or spontaneous echo contrast, in this transesophageal echocardiogram of a fibrillating left atrium are associated with prethrombotic conditions.
Protruding Atheroma in Descending Aorta Protruding atheroma (arrows) in the descending aorta (DESC AO) is evident in this transesophageal echocardiogram.
Atrial FibrillationManagement of the Risk of Stroke • Anticoagulation with warfarin is twice as effective as with Aspirin • SPAF III: compared warfarin vs. combination of low dose warfarin and aspirin - in high risk AF patients the combination was not as effective as warfarin.
Recommendations for Anticoagulation in AF • Low risk patient (younger than 65) – do not need anticoagulation • Patients above 65 years who have AF should be anticoagulated. ACP recommendation – INR 2.0 – 3.0 (reduces risk by 2/3) • Warfarin considered in younger patients with risk factors (previous TIA, HTN, CHF, Diabetes, CAD. MS, Thyrotoxicosis) • Patients, who are high risk for bleeding – give ASA 325 mg/d • Patients 65 – 75 years with no risk – balance the the low risk of stroke with side effects of therapy • Patients 75 years should receive oral anticoagulant
Atrial FibrillationManagement of the Risk of StrokeContraindications to Anticoagulation • Hemorrhage tendencies • Recent intra-cranial hemorrhage or neurosurgery • Recent hemorrhagic trauma • Recurrent or active bleeding • Diastolic BP>105 Other considerations • Risk of falling • Poor compliance with f/u • Uncontrolled siezure disorder
Atrial Fibrillation Management Cardioversion and the Risk ofThromboembolism • Risk of thromboembolism at cardioversion 0-5.6% • Dislodgement of a preexisting thrombus upon the return of the atrial electrical and mechanical function (up to 4 weeks) • Formation and later dislodgment of newly formed thrombi, when patient returns to NSR but atria in mechanical standstill • 10-15% of patients with acute AF have thrombi on TEE • Most cardioversion related thrombi do not occur at cardioversion, but are delayed for hours or weeks
Atrial Fibrillation Anticoagulation In Patients Undergoing Cardioversion • Those with A.F. longer than 2 days or of unknown duration should receive anticoagulation • Warfarin should be given 3 weeks before cardioversion and 4 weeks after cardioversion • Anticoagulation beyond 4 weeks should be considered in patients with cardiomyopathy h/o previous ambolus or mitral valve disease • TEE role in cardioversion • Useful in r/o thrombus and facilitating early cardioversion by using short term anticoagulation • Acute trial: compared TEE directed approach with brief anticoagulation to conventional
Treatment Protocol in ACUTE Study Treatment protocol used in Assessment of Cardioversion Using TEE (ACUTE) multicenter pilot study. The study involved 126 patients randomized into one of two treatment groups: the TEE guided group (62 patients) and the conventional-treatment group (64 patients).
Multifocal Atrial Tachycardia • Presents similarly to AF but arise not by multiple interlacing wavelets of reentry (as in AF) but by focal pacemaker abnormalities • The term multifocal atrial tachycardia implies several different P wave morphologies (at least 3 different morphologies) • Atrial rates range between 100 and 250 beats per minute, and the ventricular response depends on the status of AV conduction • A 1:1 P wave-to-QRS complex ratio is common with rates less than 200 beats per minute, whereas at higher rates various degrees of block (e.g., 3:2, 2:1, 3:1) are common
Multifocal Atrial Tachycardia • Causes • Chronic Obstructive Lung Disease • Any other underlying pulmonary disorders can cause MAT • Can be exacerbated by theophylline
Treatment • Treat underlying disease • Similar treatment as AF • However beta-blockers contraindicated in those whose MAT is caused by lung disease • Digoxin is not as useful and may even exacerbate the tachycardia • Use calcium channel blockers
Regular Atrial Tachycardias • 1) Sinus Tachycardia: physiologic or pathologic increase of sinus rate > 100 bpm. • Treat the condition causing the tachycardia, not the tachycardia itself. • However, in cases of acute MI sinus tachycardia must be controlled to prevent myocardial ischemia (beta blockers or Ca-channel blockers) • 2) Paroxysmal Atrial Tachycardia: sudden onset, a normal heart, HR 150-250 bpm. • P waves may be not visible because buried in the QRS complex or the T wave • Therapy: quiet setting and comfort the patient to reduce sympathetic discharge. Increase vagal tone by carotid sinus massage or valsalva maneuver. Medical therapy: Beta-blocker, Ca channel blocker, digoxin, adenosine. If angina, hypotension, or CHF then consider cardioversion.
Supraventricular Tachycardias • Atrial Tachycardia • Atrial Fibrillation/flutter • AV nodal reentry (micro) tachycardia • AV reentry tachycardia (macro) - WPW Syndrome or concealed accessory pathway If the patient is very symptomatic or breaks through drugs, consider catheter ablation
Supraventricular TachycardiaAtrioventricular Nodal Reentry Tachycardia(AVNRT) • The most common type of paroxysmal SVT (PSVT) • AVNRT accounts for 50 – 60% of PSVT • AVNRT present later than SVT related to accessory pathways (frequently after 20 years of age)
Tachycardia Induction-Reentry During sinus rhythm, antegrade conduction occurs through both the fast pathway and the slow pathway. However, the fast-pathway conduction predominates and the atrioventricular conduction time is short. If a premature atrial beat blocks in the antegrade fast pathway, atrioventricular (AV) conduction proceeds via the slow pathway. Then, if the fast pathway recovers quickly enough to permit retrograde conduction, atrial echoes or typical slow-fast atrioventricular nodal reentrant tachycardia (AVNRT) occurs. This simplified diagram demonstrates only one method of tachycardia induction and implies the requisite tachycardia circuit is confined to the compact AV node.