Download
1 / 17
360 likes | 1.92k Views
SURGICAL HIP DISLOCATION. By Sabrina Cerciello. SURGICAL HIP DISLOCATION is a demanding surgical procedure that permits unlimited access to the entire hip joint to address lesions and labral pathology. Age Consideration. Patient age is highly variable Younger patients more common

E N D
SURGICAL HIP DISLOCATION By Sabrina Cerciello
SURGICAL HIP DISLOCATION is a demanding surgical procedure that permits unlimited access to the entire hip joint to address lesions and labral pathology
Age Consideration • Patient age is highly variable • Younger patients • more common • better results • less irreversible tissue damage • Older patients • caution with patient selection d/t co-morbidities and poor bone quality • at this point in life, may be more beneficial or necessary for a Total Hip Replacement (THR)
FAI • Femoro-Acetabular Impingement • Abnormal and wearing contact between the ball and socket of the hip joint, resulting in increased friction during movement that may damage joint (ref) • Most common indication • Typically young athletic men d/t over-activity of hip joint
TYPES • Two Types • Cam • femoral head/neck deformity • cartilage delamination • acetabular cartilage lifted from underlying bone • Pincer • “over-coverage” of acetabulum • labral tear • labrum = ring of elastic tissue on rim of socket of hip joint
Pre-Operative Cam Lesion Labral Tear d/t Cam Lesion Post-Operative improved sphericity of femoral head Radiograph of 10 y.o. girl diagnosed with Perthes disease
OTHER INDICATIONS • Slipped Capital Femoral Epiphysis • separation of the femoral head from the femur at the growth plate • Perthes Disease • osteonecrosis at the femoral head • Developmental Dysplasia of the Hip (DDH) • Abnormal development of hip joint • Exostoses • extra bone growth • Hip Abnormalities
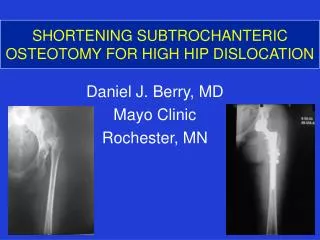
GANZ TECHNIQUE • Trochanteric Flip Osteotomy • Anterior dislocation through a posterior approach • ~1.5 cm removed and reattached with screws • Keeps external rotator muscles intact • Preserves MFCA and femoral blood supply • 2-3 hours
COMPLICATIONS • Necrosis • Nerve palsies • Infections • Adhesions • Nonunions • Hardware failures • Blood loss • RARE
POST-OP TREATMENT • TTWB or flat foot PWB • 6-8 weeks on crutches • Anti-inflammatory • NO! active abduction, passive adduction, flexion >80 degrees, external rotation • Pillow under femur • CPM 0°-30° • Seated AAROM for knee flexion/extension • May return to work in 4-6 weeks and sports in 16-24 weeks as permitted
POST-OP PHASES • Phase I • Day 1 – Week 6 • Protect surgical site, minimize pain and inflammation, patient compliance w/ activity modification • Phase II • Weeks 6 – 12 • same emphasis as Phase I • Phase III • Weeks 12 – 16 • Independent HEP, optimized ROM, 5/5 strength, pain free ADLs • Phase IV • Weeks 16 – 20 • Independent HEP, minimize post-exercise soreness
STRENGTHENING • Isometric Therex IMMEDIATELY after surgery • Ankle pumps x10 • Gluteal sets x10 • Quadriceps sets x10 • 3 sets/day • Aquatic walking at chest height~2 weeks • More intensive strengthening may begin after ~3 months • closed chain, eccentric loading, treadmill
STRETCHING • BE VERY CAUTIOUS! • starts ~3 mos. post-op • Independent ROM 1-2 years post-op • Dependent on stable pelvis • pelvis motion creates “false movement” of hip joint & no stretching is achieved • Paired with proprioception or balance work • Bosu, Biodex, single limb stance, swiss balls
HOME EXERCISE PROGRAM • Isometric Quad sets • Towel roll under knee • Ankle pumps • Abdominal sets • Abdominal control with arm motion • 2-5lbs in hand • AAROM • Knee Extension
WHY NOT A THR? • Limited access to the various specific sections of the hip joint • Inability to reshape the acetabulum • Decreased ability to meticulously reshape the femoral head • Higher risk of cartilage damage
REFERENCES • Beck, M. "Groin Pain after Open FAI Surgery: the Role of Intraarticular Adhesions.” National Center for Biotechnology Information, 10 Dec. 2008. Web. Retrieved 10 Oct. 2012. <http://www.ncbi.nlm.nih.gov/pubmed/19082679>. • “Femoro-Acetabular Impingement (FAI).” The Hospital for Special Surgery. Retrieved 20 Oct. 2012. <http://www.hss.edu/condition-list_hip-impingement-femoroacetabular-impingement.asp>. • Ganz, R., T. J. Gill, E. Gautier, K. Ganz, N. Krugel, and U. Berlemann. "Surgical Dislocation of the Adult Hip." Jbjs.org. The Journal of Bone and Joint Surgery, Nov. 2001. Web. 13 Retrieved Oct. 2012. • Jamali, Amir. (2010) Surgical Hip Dislocation. Retrieved 11 Oct. 2012. Joint Preservation Institute web site. <http://www.jointpreservationinstitute.com/faq-surgical-hip-dislocation.html> • Krueger, Andreas, Michael Leunig, Klaus A. Siebenrock, and Martin Beck. "Hip Arthroscopy After Previous Surgical Hip Dislocation for Femoroacetabular Impingement.” Science Direct, Dec. 2007. Web. Retrieved 10 Oct. 2012. <http://www.sciencedirect.com/science/article/pii/S0749806307006688>. • Munting, T.W. Open Hip Dislocation (Debridment) Surgery. Retrieved 13 Oct. 2012. Cape Town Sports and Orthopedic Clinic web site. <http://www.ctorth.com/dr-munting/open-hip-surgery.html> • Peters, Christopher L., and Jill A. Erickson. "Treatment of Femoro-Acetabular Impingement with Surgical Dislocation and Débridement in Young Adults.” Journal of Bone and Joint Surgery, 2006. Web. Retrieved 11 Oct. 2012. <http://www.jbjs.org/article.aspx?Volume=88>. • Ray, Linda. (2011) Hip Dislocation Surgery and Rehabilitation. Retrieved 11 Oct. 2012. Livestrong. <http://www.livestrong.com/article/426593-hip-dislocation-surgery-rehabilitation/> • Rebello, Gleeson, Samantha Spencer, Michael Millis, and Young-Jo Kim. "Surgical Dislocation in the Management of Pediatric and Adolescent Hip Deformity.” National Center for Biotechnology Information, U.S. National Library of Medicine, 6 Oct. 2008. Web. Retrieved 12 Oct. 2012. <http://www.ncbi.nlm.nih.gov/pmc/articles/PMC2635463/?tool=pubmed>. • Sink, E. “Surgical Hip Dislocation.” Orthopedics. May 2009. Retrieved 11 Oct. 2012. <http://www.healio.com/orthopedics/journals/ortho/%7Bd7a2e1ac-d7d5-4d3c-8e52-8a713f0e4218%7D/surgical-hip-dislocation>.