Download
1 / 22
230 likes | 851 Views
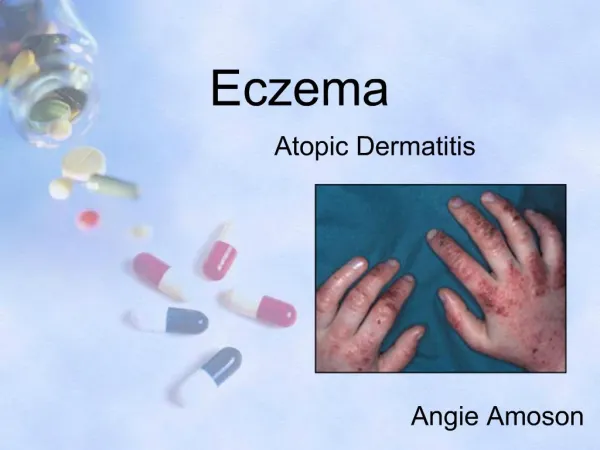
ECZEMA. DR SIVANIE VIVEHANANTHA DERMATOLOGY STR. AIMS. Brief overview of eczema Enable early recognition & effective management. ECZEMA. CLASSIFICATION OF ECZEMA. ENDOGENOUS Atopic Seborrheic Discoid Pompholyx / dyshidrotic Varicose / venous / stasis / gravitational. EXOGENOUS

E N D
ECZEMA DR SIVANIE VIVEHANANTHA DERMATOLOGY STR
AIMS • Brief overview of eczema • Enable early recognition & effective management
CLASSIFICATION OF ECZEMA ENDOGENOUS • Atopic • Seborrheic • Discoid • Pompholyx / dyshidrotic • Varicose / venous / stasis / gravitational EXOGENOUS • Allergic contact • Irritant contact • Photosensitive / photoaggravated
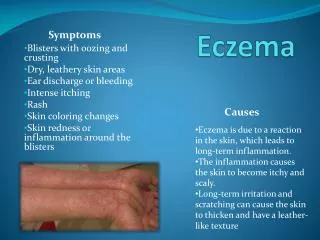
MANAGEMENT OF EXOGENOUS EZCEMA • Avoidance of offending agent • Topical steroids +/- prednisolone • Patch testing for allergic contact dermatitis or photo-patch testing for photo-allergic dermatitis • Soap substitutes and emollients
HISTORY • Age of onset? • H/O childhood eczema? • Any evidence of worsening eczema with diet? If so, which type of food? • Areas affected? • Worsening / improving / static disease? • Eczema free days? • Pruritus? If so, does it keep the patient up at night? • Antibiotics? Hospitalisation for infective flare ups? • H/O eczema herpeticum? • H/O erythroderma?
PMH: Atopy? • FH: - Atopy? - Ask specifically if any siblings. If has siblings, atopy? • DH: - What meds? - Previous treatments? Helpful / unhelpful? - Current treatment? Helpful / unhelpful? - Always ask about: • Frequency of application and quantities used! • SS , shampoo, emollient, topical steroid, steroid sparing agent, scalp applications, suits, antihistamines • Days off school / work?
MANAGEMENT • Bath additives (antibacterial?) • Soap substitute (antibacterial?) and shampoo • Emollient • Topical steroid (combination with topical antibiotic?) • Steroid sparing agents eg. topical tacrolimus • Scalp application • Potassium permanganate soaks
Suits • Bandaging eg. viscopaste, tubigrip • Antihistamines (driving advice!) • Allergen avoidance • Dietitician involvement? • Occupational health involvement • IgE levels? (inteprete with caution!) • Systemic treatment eg. prednisolone, ciclosporin etc
Tailor treatment to each INDIVIDUAL patient’s needs and adapt management plan to increase compliance! • Remember Afrocaribbean / Black people only wash their hair once a week and may be reluctant to use certain topical treatment if hair relaxed. Ask patient if they are willing to change hairstyle. • Nurse involvement in skin care regimen • REMEMBER: 1 FTU = 0.5 grams = Covers surface area equivalent to 2 palms Ensure patient is aware of this and prescribe adequate amounts of topical treatment!
ERYTHRODERMA • > 90% involvement of inflammatory skin disease • Causes: - Eczema - Psoriasis - CTCL (Sezary syndrome) - Drugs - Lymphoma / leukaemia - GvHD - HIV - Idiopathic
Consequences: - Heat loss - Fluid loss (Hypovolaemia and renal failure) - Electrolyte imbalance - High output cardiac failure - Hypoalbunaemia - Hyperuricaemia - Death! • Mx (Symptomatic): - Rx underlying condition / remove offending drug - Temperature control - IV fluids - Dietician input +/- ITU admission
SUMMARY • Brief overview of eczema • Early recognition and effective management • Early involvement of Dermatologist when eczema is poorly controlled +/- erythrodermic or if patch test is required