Download
1 / 2
20 likes | 87 Views
Introduction The Radiological Physics Center (RPC) provides QA services to over 1,800 institutions (~14,000 beams) in the United States and internationally that consist of: Evaluating radiotherapy programs Developing protocols and QA procedures Helping to correct institutional deficiencies

E N D
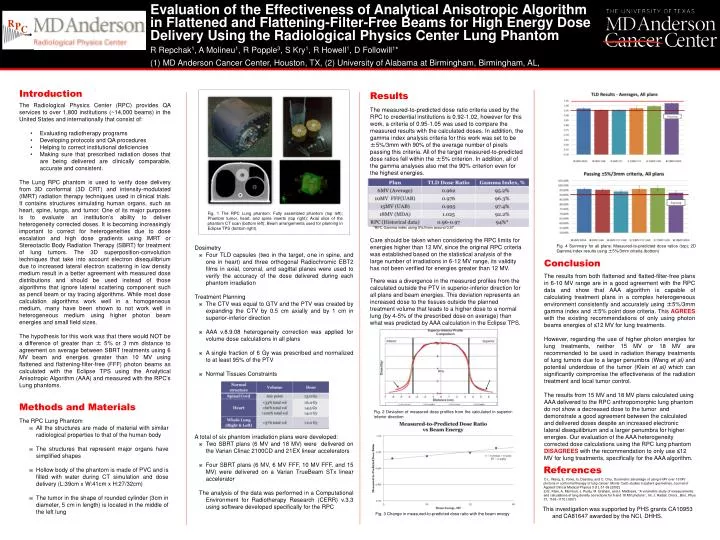
Introduction • The Radiological Physics Center (RPC) provides QA services to over 1,800 institutions (~14,000 beams) in the United States and internationally that consist of: • Evaluating radiotherapy programs • Developing protocols and QA procedures • Helping to correct institutional deficiencies • Making sure that prescribed radiation doses that are being delivered are clinically comparable, accurate and consistent. The Lung RPC phantom is used to verify dose delivery from 3D conformal (3D CRT) and intensity-modulated (IMRT) radiation therapy techniques used in clinical trials. It contains structures simulating human organs, such as heart, spine, lungs, and tumor. One of its major purposes is to evaluate an institution’s ability to deliver heterogeneity corrected doses. It is becoming increasingly important to correct for heterogeneities due to dose escalation and high dose gradients using IMRT or Stereotactic Body Radiation Therapy (SBRT) for treatment of lung tumors. The 3D superposition-convolution techniques that take into account electron disequilibrium due to increased lateral electron scattering in low density medium result in a better agreement with measured dose distributions and should be used instead of those algorithms that ignore lateral scattering component such as pencil beam or ray tracing algorithms. While most dose calculation algorithms work well in a homogeneous medium, many have been shown to not work well in heterogeneous medium using higher photon beam energies and small field sizes. The hypothesis for this work was that there would NOT be a difference of greater than ± 5% or 3 mm distance to agreement on average between SBRT treatments using 6 MV beam and energies greater than 10 MV using flattened and flattening-filter-free (FFF) photon beams as calculated with the Eclipse TPS using the Analytical Anisotropic Algorithm (AAA) and measured with the RPC’s Lung phantoms. • Methods and Materials • The RPC Lung Phantom • All the structures are made of material with similar radiological properties to that of the human body • The structures that represent major organs have simplified shapes • Hollow body of the phantom is made of PVC and is filled with water during CT simulation and dose delivery (L:39cm x W:41cm x H:27/32cm) • The tumor in the shape of rounded cylinder (3cm in diameter, 5 cm in length) is located in the middle of the left lung Evaluation of the Effectiveness of Analytical Anisotropic Algorithm in Flattened and Flattening-Filter-Free Beams for High Energy Dose Delivery Using the Radiological Physics Center Lung Phantom R Repchak1, A Molineu1, R Popple3, S Kry1, R Howell1, D Followill1* (1) MD Anderson Cancer Center, Houston, TX, (2) University of Alabama at Birmingham, Birmingham, AL, Results The measured-to-predicted dose ratio criteria used by the RPC to credential institutions is 0.92-1.02, however for this work, a criteria of 0.95-1.05 was used to compare the measured results with the calculated doses. In addition, the gamma index analysis criteria for this work was set to be ±5%/3mm with 90% of the average number of pixels passing this criteria. All of the target measured-to-predicted dose ratios fell within the ±5% criterion. In addition, all of the gamma analyses also met the 90% criterion even for the highest energies. *RPC Gamma index using 5%/5mm around 0.97 Care should be taken when considering the RPC limits for energies higher than 12 MV, since the original RPC criteria was established based on the statistical analysis of the large number of irradiations in 6-12 MV range, its validity has not been verified for energies greater than 12 MV. There was a divergence in the measured profiles from the calculated outside the PTV in superior-inferior direction for all plans and beam energies. This deviation represents an increased dose to the tissues outside the planned treatment volume that leads to a higher dose to a normal lung (by 4-5% of the prescribed dose on average) than what was predicted by AAA calculation in the Eclipse TPS. Fig. 1 The RPC Lung phantom: Fully assembled phantom (top left); Phantom tumor, heart, and spine inserts (top right); Axial slice of the phantom CT scan (bottom left); Beam arrangements used for planning in Eclipse TPS (bottom right). • Dosimetry • Four TLD capsules (two in the target, one in spine, and one in heart) and three orthogonal Radiochromic EBT2 films in axial, coronal, and sagittal planes were used to verify the accuracy of the dose delivered during each phantom irradiation • Treatment Planning • The CTV was equal to GTV and the PTV was created by expanding the CTV by 0.5 cm axially and by 1 cm in superior-inferior direction • AAA v.8.9.08 heterogeneity correction was applied for volume dose calculations in all plans • A single fraction of 6 Gy was prescribed and normalized to at least 95% of the PTV • Normal Tissues Constraints • A total of six phantom irradiation plans were developed: • Two SBRT plans (6 MV and 18 MV) were delivered on the Varian Clinac 2100CD and 21EX linear accelerators • Four SBRT plans (6 MV, 6 MV FFF, 10 MV FFF, and 15 MV) were delivered on a Varian TrueBeam STx linear accelerator • The analysis of the data was performed in a Computational Environment for Radiotherapy Research (CERR) v.3.3 using software developed specifically for the RPC Fig. 4 Summary for all plans: Measured-to-predicted dose ratios (top); 2D Gamma index results using ±5%/3mm criteria (bottom) Conclusion The results from both flattened and flatted-filter-free plans in 6-10 MV range are in a good agreement with the RPC data and show that AAA algorithm is capable of calculating treatment plans in a complex heterogeneous environment consistently and accurately using ±5%/3mm gamma index and ±5% point dose criteria. This AGREES with the existing recommendations of only using photon beams energies of 12 MV for lung treatments. However, regarding the use of higher photon energies for lung treatments, neither 15 MV or 18 MV are recommended to be used in radiation therapy treatments of lung tumors due to a larger penumbra (Wang et al) and potential underdose of the tumor (Klein et al) which can significantly compromise the effectiveness of the radiation treatment and local tumor control. The results from 15 MV and 18 MV plans calculated using AAA delivered to the RPC anthropomorphic lung phantom do not show a decreased dose to the tumor and demonstrate a good agreement between the calculated and delivered doses despite an increased electronic lateral disequilibrium and a larger penumbra for higher energies. Our evaluation of the AAA heterogeneity corrected dose calculations using the RPC lung phantom DISAGREES with the recommendation to only use 12 MV for lung treatments, specifically for the AAA algorithm. Fig. 2 Deviation of measured dose profiles from the calculated in superior-inferior direction References 1) L. Wang, E. Yorke, G. Desobry, and C. Chui, Dosimetric advantage of using 6 MV over 15 MV photons in conformal therapy of lung cancer: Monte Carlo studies in patient geometries, Journal of Applied Clinical Medical Physics 3 (1), 51-59 (2002) 2) E. Klein, A. Morrison, J. Purdy, M. Graham, and J. Matthews, ‘‘A volumetric study of measurements and calculations of lung density corrections for 6 and 18 MV photons’’, Int. J. Radiat. Oncol., Biol., Phys. 37, 1163–1170 (1997) This investigation was supported by PHS grants CA10953 and CA81647 awarded by the NCI, DHHS. Fig. 3 Change in measured-to-predicted dose ratio with the beam energy
Title of the Poster Presentation Goes Here Authors of the Poster Presentation Goes HereInstitutional and/or Graduate School of Biomedical Sciences Affiliation Goes Here Title of the Poster Presentation Goes Here Authors of the Poster Presentation Goes HereInstitutional and/or Graduate School of Biomedical Sciences Affiliation Goes Here Title of the Poster Presentation Goes Here Authors of the Poster Presentation Goes HereInstitutional and/or Graduate School of Biomedical Sciences Affiliation Goes Here Title of the Poster Presentation Goes Here Authors of the Poster Presentation Goes HereInstitutional and/or Graduate School of Biomedical Sciences Affiliation Goes Here Title of the Poster Presentation Goes Here Authors of the Poster Presentation Goes HereInstitutional and/or Graduate School of Biomedical Sciences Affiliation Goes Here Title of the Poster Presentation Goes Here Authors of the Poster Presentation Goes HereInstitutional and/or Graduate School of Biomedical Sciences Affiliation Goes Here Title of the Poster Presentation Goes Here Authors of the Poster Presentation Goes HereInstitutional and/or Graduate School of Biomedical Sciences Affiliation Goes Here Title of the Poster Presentation Goes Here Authors of the Poster Presentation Goes HereInstitutional and/or Graduate School of Biomedical Sciences Affiliation Goes Here Title of the Poster Presentation Goes Here Authors of the Poster Presentation Goes HereInstitutional and/or Graduate School of Biomedical Sciences Affiliation Goes Here Title of the Poster Presentation Goes Here Authors of the Poster Presentation Goes HereInstitutional and/or Graduate School of Biomedical Sciences Affiliation Goes Here






















