Download

1 / 14
160 likes | 651 Views
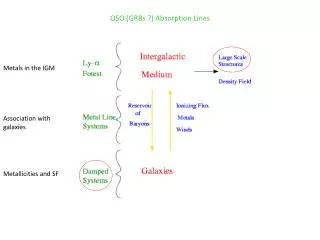
ImmunoDOT. Leptospira IgM. Leptospirosis. Possible alternative diagnoses to consider will include : Viral hepatitis Meningitis Influenza Malaria Typhoid fever Yellow fever Relapsing fever Scrub typhus Dengue fever Legionnaires' disease

E N D
ImmunoDOT Leptospira IgM
Leptospirosis • Possible alternative diagnoses to consider will include: • Viral hepatitis • Meningitis • Influenza • Malaria • Typhoid fever • Yellow fever • Relapsing fever • Scrub typhus • Dengue fever • Legionnaires' disease • Toxic shock syndrome Leptospirosis is a disease caused by pathogenic spirochetes of the genus Leptospira. It is considered the most common zoonosis in the world. Infection may cause no symptoms, a mild flu-like illness, or a more severe illness with jaundice and kidney failure (Weil's disease). Leptospira can be cultured , but the median time to positivity is three weeks with a maximum of three months. This makes culture techniques useless for diagnostic purposes.
Microscopic Agglutination Test (MAT) • Used by public health agencies • Used to define serovars within the population • When testing IgM only, there is significant cross-reactivity between serovars. However the MAT test, detects both IgG and IgM, and therefore detects differences between serovars. • MAT is primarily used to classify the organism. This is useful for public health purpose, but of little important for patient diagnosis.
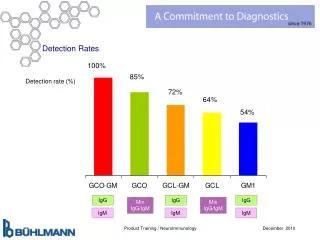
IgM versus MAT Sensitivity IgM (EIA) MAT (IgG and IgM) Acute Specimen 1 = 30% Acute Specimen 2 = 63% Convalescent Specimen = 76% • Acute Specimen 1 = 52% • Acute Specimen 2 = 89% • Convalescent Specimen = 93% Cumberland, P. C., C. O. R. Everard, and P. N. Levett. 1999. Assessment of the efficacy of the IgM enzyme-linked immunosorbent assay (ELISA) and microscopic agglutination test (MAT) in the diagnosis of acute leptospirosis. Am. J. Trop. Med. Hyg. 61:731–734.
Leptorapide (Rapid Assay) • Intended use is the detection of total antibody. The kit does not have FDA clearance to claim detection of Leptospira specific IgM. • Test claims that performance is the same as MAT test (see previous MAT slide) • Unlike an IgM specific test, this total antibody test requires acute and convalescent specimen for diagnosis (2 specimens collected weeks apart) • Kit may be used for epidemiology purpose, but single specimen diagnosis is not allowed based on the kit’s intended use.
Specimen Collection • When the specimen is taken early, the interval between paired samples may be short (2-4 days). • Since the early symptoms of leptospirosis are often regarded as non-specific, in many poorer rural populations, where medical attention may be both difficult to obtain and costly, it is less likely that early acute-phase samples will be taken. • If patients are not ill enough to require hospitalization, then a longer interval between samples may be appropriate.
Laboratory Validation ImmunoDOT
ImmunoDOT Leptospira IgM • IgM Enzyme Immunoassay (EIA) • A semi quantitative assay, with each extra dot representing an approximately fourfold increase in titer. Thus it is possible to detect both seroconversion and a rising titer of IgM antibodies. • Detects all pathogenic Leptospira serovars • Easy to use • Digital record (picture)
Initial Validation – GenBio Panel • Contact GenBio for known positive specimen. • Assure test performs as expected using sera collected from the local population(s) • Assure technicians understand the testing procedure • Determine how to report results to clinicians
Validation Panel Example of an ideal validation panel. Availability is limited. Contact GenBio for more information. Level 1 = 3 strong dots Level 2 = 2 strong dots Level 3 = 2 strong dots Level 4 = 1+ strong dots Level 5 = Weak reaction If the laboratory observes similar reactivity, positive reactivity is verified.
Local IgM Prevalence • It is important that the laboratory and clinicians understand the prevalence of Leptospira IgM in healthy, uninfected subjects. Most populations report no dots or a weak one dot ImmunoDOT reactivity. • GenBio recommends testing 20 to 50 sera collected from healthy adults. • If a specific population (e.g., agricultural workers, pediatrics) represents a significant portion of the intended population, assure specimens from this population are included in the study.
Interpretation Methods • Assure technicians are aware of prevalence results. It may be useful to take a picture of reacted assays strips that represent “low” reactivity within the local population. These can be used to train technicians how provide interpretation support to the clinician. • For comparison, a digital record (picture) is useful when interpreting subsequently collected serum (acute/convalescent serum pairs). • Pictures can be taken using most cameras or smart phones. It is best to take pictures using the same a similar light condition.
Negative or Strong Positive Result • Negative results do not rule out the diagnosis of leptospirosis. The specimen may have been drawn before the appearance of detectable antibodies. • Three (3) strong dots are a good indication current infection, assuming the patient’s signs and symptoms are consistent with Leptospirosis. Testing a specimen collected several days later and observing increased reactivity provides additional support. If available, the MAT method may be used to affirm the result and provide serovar information.
Less than 3 Dot Results • Interpret less intense reactions with caution. • Prevalence of less intense reactions within the population can be useful when providing a clinical interpretation result. • Patient signs and symptoms are always important when interpreting serology results. • Specific IgM can remain for weeks to months after infection, so presence of IgM alone (no significant signs or symptoms) are never sufficient for diagnosis.