Download
1 / 24
240 likes | 280 Views
February – March 2006 Group A Streptococcus Necrotizing Fasciitis Outbreak in Johnson County. Lyle Snider, Ph.D. Big Sandy Regional Public Health Epidemiologist ERRT Conference Dec. 14, 2006, Frankfort, KY. Summary of Case A. Case A

E N D
February – March 2006 Group A Streptococcus Necrotizing Fasciitis Outbreak in Johnson County Lyle Snider, Ph.D. Big Sandy Regional Public Health Epidemiologist ERRT Conference Dec. 14, 2006, Frankfort, KY
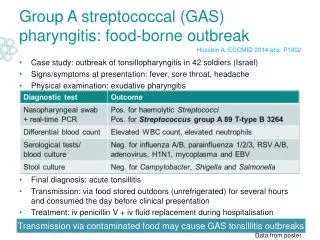
Summary of Case A • Case A • March 1st: 73 yr-old female drove from Paintsville to Lexington in the afternoon. Grandaughter Noted Red, Warm, & Raised Area on Back in the Evening • March 2nd: Lexington Hospital ER in AM, Lapsed into coma in PM • April 1st: Case Died
Summary of Case B • Case B • March 8th: 33 yr-old Female walked into Paintsville ER in AM with abscess on breast. Lapsed into Coma & Coded in ER. Helicopter ride to Cabell Huntington Hospital during which she coded again. • March 23rd: Case Died
Format Derived fr p. 41-3, KY Reportable Dis. Desk Ref Reason for Investigation, Brief statement as to how outbreak became known. • March 8th, AM, when Case B presented in Paul B Hall ER, coded, was helicoptered, etc., the Hospital Nursing Dir./Infection Control Nurse called Johnson Co HD (JCHD) right away to report Case B, and to tell her of the rumor of another case in the area. • March 8th, 1:41 PM, Teresa Lawson, ARNP, JCHD Infection Control, send me a brief e-mail about the case sent to WV, and the rumor of a 2nd case. • Hospital Infection Control Nurse enters case on March 8th, 2 PM.
How We Learned of Case A • March 8th – Rumor & e-mail to me • March 9th, Case A’s daughter left message on Div. of Epid’s evening message system that her mother may have necrotizing fasciitis March 9th, and that she had heard that there were other cases aroundPaintsville. • March 9th - Case entered in DSM March 9th at 4:43 PM by hospital infection control nurse. • March 10th - Call from Dr. Brawley to Ms. Lawson confirming 2nd Case. She then called me on cell in Bristol, TN at Public Health meeting.
Public Information • March 9th - word of the 2 cases of the “flesh-eating disease” were spreading throughout the community. • Ms. Lawson, Russell Briggs (Dir. Of JCHD), and Dr. Brawley composed a brief press release. • Mr. Briggs discussed it informally with parents at an elementary school health fair • At least 2 TV Interviews, one by Ms. Lawson, one by me - Hazard/Lex. CBS and WV NBC (?)
More Public Information • March 11th – Lex. Herald Leader Around KY 1-paragraph report entitled Two Incidents of Kissing Disease. • Lead sentence reads, “Health officials in Johnson Co issued a warning yesterday concerning a so-called “kissing disease” that has hospitalized 2 residents this month.” • The rest of the article was taken directly from the press release.
1999-2005 KY Invasive Gr A Streptococcus Incidence Frequency KY Case Rate Range 0.6 – 1.5 Cases/100,000 Population Johnson Co population ~ 24,000 Necrotizing Fasciitis is not a reportable disease
Invasive Gr A Streptococcus (GAS) Communicability • Reservoir of Gr A Streptococcus Organism is Humans • Incubation Period, 1 – 3 days • Mode of Transmission: Large Respiratory Droplets or Direct Contact With Infected Person • Rarely spread through indirect contact (WalMart cart handles) • Gr A Strep Necrotizing Fasciitis wound drainage and secretions are infective • Control of Comm Diseases says 24 hrs of effective antibiotic treatment ends infectivity (??) • Mortality Rate – 10 – 13%
Necrotizing Fasciitis • Skin and Soft Tissue are Destroyed • Is caused by several different organisms • Organisms Spread Along Superficial & Deep Fascial Planes – helped by bacterial enzymes & toxins • Leads to vascular occlusion, ischemia, and tissue necrosis • May lead to overwhelming systemic sepsis • Mortality Rate ~ 25%
Investigation • Entered Info from Hospitals in DSM • History of Disease in Cases • Health Status Prior to Disease • When did symptoms 1st appear, and how did disease progress? • Formulated survey form w Dr. Brawley to interview family, friends, co-workers, etc. • Did 1 Case “Catch” This From Another Case? • Are there other cases in the community?
Pulse-field Gel Electrophoresis (PFGE) Results • No detectable difference in the bacteria (i.e. both women were infected with the same strain of the bacteria). • Reports from Iowa and Massachusetts indicate that the PFGE pattern in these two cases is more common than any other pattern. • The PFGE pattern was found in 35 of ~ 150 (~25%) cases of Massachusetts Group A Streptococcus invasive disease, and two of three cases in Iowa
Case A Health Status and Development of Disease • 73 yr old works part time in department store, and drove 100+ miles by herself fr Paintsville to Lexington to care for granddaughter • Cared for grandchildren after school • Had Rheumatoid Arthritis and Took Methotrexate for it • Symptoms developed suddenly: couldn’t get shirt off by herself, granddaughter noted lesion, in a coma less than 24 hours later
Case B Health Status and Development of Disease • 33 yr old, married living with husband and child (elementary school-age) • Office Worker in a Small Factory • Long History of Superficial skins lesions that she treated with antibiotic ointment & pain pills • Frequent recent absences from work related to own flu-like illnesses and child’s ear aches, etc.
Investigation Tools • Map of Case Homes • Survey Instrument for Interviews • Interviews • Genograms • Timelines
Case A Downtown Paintsville 1-2 Blocks from the Johnson Co Health Dept. & Paul B Hall Hospital Case B Near Van Lear ~ 4 Miles Between Homes As the Crow Flies
Date Case B, 33 yrs old Case A, 74 yr old Jan 17 Saw rheumatologist in Pikeville. He renewed methotrexate prescription, 2.5 mg, five pills once a week. He also ordered basic liver function and blood cell tests. Jan 28 Started work at Peebles Mon Feb 6 – Thurs Feb 9 Worked four 8-hour days at factory. Seen by several at Dr. XYZ’s funeral and appeared to be in good health. She worked in his office for many years before his retirement. Survey Instrument for Interviews
Interviews • See Word Document • Major Limitation of Interviews • Case A’s Family Refused to be Interviewed after 2nd – 3rd Day of Contact
Father died of disease A. • Mother too upset about Case B’s death to be interviewed, according to her sisters. • Case’s Aunt One staying at Mother’s house when Aunt One was interviewed on April 12th Genogram Case B’s Gr Mother Case B’s Gr Father Aunt Two Aunt One Mother Father Both Work at XYZ Hospital Case B Husband • Jane XXX-XXXX, Case’s Friend • Jane’s Boyfriend is Sam Smith • Case & Husband worked at XYZ factory. • Case’s Supervisor, XXX-XXXX 1st Son ~ 16 yrs old 2nd Son ~ 8 yrs old
Time Line Date Case A, 74 yrs old Case B, 33 yrs old Saw rheumatologist in Pikeville. Renewed prescription. Ordered liver function and blood cell tests. Jan 17 Started work at Peebles Jan 28 Worked four 8-hour days at factory. Feb 6 – 9
Discussion as to Source • No Contact Between Cases Discovered During Interviews • Lots of rumors in community about a family restaurant • No Other Invasive Gr A Streptococcus Infections discovered in Johnson Co or neighboring counties.
Conclusions • No connection between cases was found. • Unable to Interview Family Members and Community Members Who May Have Known Information Related to Source of Infection. • Need to Establish Hospital Reporting Behavior on accreditation surveys.
Summary of Control Measures • Risk of acquiring infection from Cases was vanishingly small UNLESS One Has Immune Deficiency, or Other Debilitating Illness. • If in doubt about need for prophylaxis, consult your physician (Case A’s sister did this).
Indispensable Collaborators • Teresa Lawson, ARNP, Johnson Co. Health Department Infection Control Nurse • Robert Brawley, MD, • Sandy Kelly, RN • Family Members, Hospital Infection Control Nurses, Case Employers, Friends of Cases