Download
1 / 17
170 likes | 183 Views
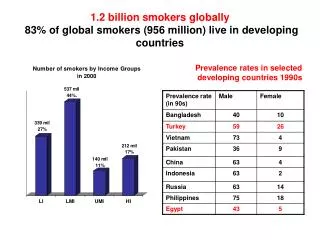
Explore the state-of-the-art strategies for treating smokers, addressing motivation to smoke, treatment goals, effectiveness, and future advancements. Learn about treatment targets, outcome assessment, and diverse treatment options featuring various medications and support programs.

E N D
Behavioural and pharmacological approaches to treating smokers: the state of the art Robert West University College London WCTOH Washington 2006
Outline • The need for treatment • The goals of treatment • The effectiveness of treatment • The future of treatment
The need for treatment • Repeated nicotine from cigarettes interacts with other smoking stimuli to generate: • impulses to smoke generated by smoking cues • a ‘drive’ to smoke somewhat resembling hunger • unpleasant physical and psychological symptoms associated with not smoking • feelings of attraction to smoking • positive evaluations of smoking • These act at all levels of the motivational system and overwhelm, undermine and subvert self-conscious decisions to become a non-smoker
Motivation to smoke Smoking Cues Impulse to smoke Anticipated enjoyment Nicotine ‘hunger’ Desire to smoke Need to smoke Adverse mood and physical symptoms Expected benefit Positive evaluation of smoking Smoker ‘identity’ Functional beliefs Derived from PRIME Theory of motivation: www.primetheory.com
The role of treatment • After some days or weeks of abstinence most of these motivational forces tend to diminish in frequency and intensity, but ... • the rate of decay is variable • upsurges are common • sometimes they persist indefinitely • The goal of treatment: • to keep the moment-to-moment motivation to smoke lower than the motivation to to at all times until the motivational system ‘recovers’
Schematic of the moment-to-moment flux of motivation to smoke Action threshold (restraint, competing motives) Lapses Impulse to smoke Day 1 Day 2 Day 5 Day 10 Day 20
Potential treatment targets • Minimising frequency and intensity of motivation to smoke: • Minimise the strength of the drive to smoke • Minimise frequency and intensity of cue-driven impulses to smoke • Minimise adverse mood and physical symptoms • Undermine smoker identity • Undermine functional beliefs about smoking • Foster adaptive mental or physical responses to smoking triggers • Raising the action threshold • Maximise social pressure not to smoke • Maximise negative feelings about smoking (disgust, worry etc.) • Foster an ‘in-control’, ‘non-smoker’ identity • Foster functional beliefs about not smoking • Preserve mental energy needed for self-control • Foster alternative behaviours
Assessing treatment outcome • Ultimate goal is usually ‘permanent remission’ (Peter Selby) • Self-report of continuous abstinence for 6 months, biochemically verified, usually allows reliable estimation of this (Russell Standard1) • permanent remission rate~50% RS6M • ‘Point-prevalence’ estimation and estimation for shorter time periods are less reliable • The key effect-size measure is difference in the proportion of smokers abstinent in treatment versus control conditions 1West et al, Addiction 2005
Effect of face-to-face individual support Using only studies with ≥6 months’ continuous abstinence and biochemical verification
Effect of group support Using only studies with ≥12 months’ continuous abstinence and biochemical verification
Effect of telephone counselling Cochrane review, in preparation: >6 month cessation not validated
Effect of tailored internet support Not biochemically verified
Effect of NRT Cochrane: LI: Low intensity behavioural support; HI: High intensity behavioural support RTS: Reduce To Stop; Combination: various combinations versus single NRT types; Population: NRT versus no NRT in population samples without behavioural support (ATTEMPT – cohort study, not RCT)
Effect of nortriptyline, bupropion and varenicline For bupropion and nortriptyline data from Cochrane: ≥6 months’ continuous abstinence and biochemical verification; varenicline 6 month continuous abstinence data from JAMA 2006; blue shading shows effect on 12 month continuous abstinence rates of further 12w varenicline vs placebo in smokers abstinence at 12w
Treatment options • Enrol in a structured, multi-session face-to-face or telephone-based behavioural support programme and (unless contra-indicated): • take varenicline for 12 weeks or longer if required, or • take nicotine patch for 2 weeks prior to quit date then and patch plus an acute form prn for 8 weeks or longer as required, or • take bupropion for 1-2 weeks prior to quit date and then for up to 8 weeks • Use Rx medications under clinical supervision with additional help packages supplied • Use NRT OTC with help packages supplied
Costs and benefits • Costs • Treatments to aid cessation carry very low risk • Behavioural treatments require some investment of time and effort on part of smokers • Side effects of medications vary but are generally mild • Cost per treatment episode could range from $200 for medication or behavioural support only to $800 for extended combined treatment • Benefits • Approximately 2 to 10 percentage point improvement in chances of ‘permanent remission’ (50% of effect on 6m abstinence) • Most successful quitters arising from the treatment gain an average of 3 to 6 healthy life years depending on their age and current state of health
The future of treatment • More effective use of existing treatments • combinations • pre-treatment • longer term use if required • wider access • Better treatments • novel medications • cheaper medications • more comprehensive behavioural treatments • A realistic goal • 25% of quit attempts that would have failed, lasting for at least 6 months