Download
1 / 21
220 likes | 543 Views
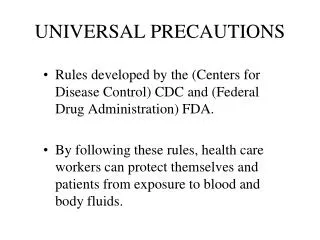
2. Project in Process. RationaleProcessPrototypeFeasibility. 3. Rationale. Low health literacy is commonWe do not have good strategies for knowing who is struggling with health informationHealth literacy universal precautions isstructuring the delivery of care in the practice as if every pati

E N D
1. 1 Developing a Health Literacy Universal Precautions Toolkit DeWalt DA, Hawk V, Broucksou K, Hink A, Brach C, Callahan LF
AHRQ Annual Meeting 2009
2. 2 Project in Process Rationale
Process
Prototype
Feasibility
3. 3 Rationale Low health literacy is common
We do not have good strategies for knowing who is struggling with health information
Health literacy universal precautions is
structuring the delivery of care in the practice as if every patient may have limited health literacy
4. 4 Process Identify and review tools
Identify gaps
Develop plan for toolkit organization
Create implementation guidance
Test individual tools
Create �toolkit� as unified approach
Pilot test toolkit in practices
5. 5 Tool identification and review Searched the internet via Google (health literacy, health communication, health education materials)
Directed inquiries: Advisory Board, Health Literacy List Serve, primary care practices in PBRN
Conducted conference calls with practices in NC and across the country with a reputation for working on health literacy universal precautions
6. 6 Tool Review Catalogued tools
Training for clinicians and staff
System changes in practices
Use of educational media
Connections with community organizations
Made assessment of how tool could be used in primary care
Ease of use
Documented experience or research on tool
Format (book, internet, video, etc)
Avoided creating a catalog of patient education materials
7. 7 Results This table is a summary of what we found.
We identified 219 candidate tools. Many tools were focused on health literacy training for providers and were generally repetitive in terms of their content. a few tools had recommended system changes, many tools were different types of educational media for patients or instructions on how to improve educational media.
A smaller number of tools were related to community linkages and other areas.
In terms of the target audience, most tools were targeted for providers and staff to improve their attention toward health literacy issues. Some were targeted toward patients, and often these were tools to encourage patients to ask questions or specific educational materials.
The other category often included policymakers or researchers that might be the target audience.This table is a summary of what we found.
We identified 219 candidate tools. Many tools were focused on health literacy training for providers and were generally repetitive in terms of their content. a few tools had recommended system changes, many tools were different types of educational media for patients or instructions on how to improve educational media.
A smaller number of tools were related to community linkages and other areas.
In terms of the target audience, most tools were targeted for providers and staff to improve their attention toward health literacy issues. Some were targeted toward patients, and often these were tools to encourage patients to ask questions or specific educational materials.
The other category often included policymakers or researchers that might be the target audience.
8. 8 Gaps to Fill Practice assessment for primary care
Individual tools (form templates for practices, patient follow-up procedures, etc.)
Implementation guidance
9. 9 Implementation Guidance How do we take an idea and get it implemented reliably and sustainably in practice?
Steps for implementation
Frame in the Model for Improvement (PDSA)
Examples of how others have done it
Ways to track progress
10. 10
11. 11
12. 12
13. 13 Test Individual Tools Each �tool� or �implementation guidance� was tested in 2-4 practices
Practices reviewed the tool and attempted implementation on a small scale
Reviewed feedback by conference call
Received feedback from Advisory Board
14. 14 Create Prototype Toolkit Developed the framework for the toolkit
Introduction
Getting Started
Form a team
Assess your practice
Raising awareness in your practice
Built in tutorial for Model for Improvement
Added examples of practices doing this work
15. 15 Toolkit Organization Introduction and getting started
Assessment of practice
Four Key Changes
Effective Oral Communication
E.g. teach back method
Effective Written Communication
E.g., forms, education materials
Self-Management and Empowerment
E.g., action plans, encouraging questions
Supportive Systems
E.g., community resources, supportive systems
16. 16 Final List of Tools Getting Started
Forming a team
Assessing your practice
Raising awareness
Effective Oral Communication
Communicating Clearly with patients
Using the teach back method
Following-up with patients
Improving telephone communication
Using the brown bag review
Addressing language differences
Knowing your patients: understanding differences
Effective Written Communication
Designing easy to understand forms
Using effective health education
Making your practice easy to navigate
Creating a welcoming front desk
Self-Management and empowerment
Encouraging questions
Action plans
Improving medication adherence
Obtaining patient feedback
Supportive systems
Providing support for patients
Getting patients the medications they need
Using health resources in your community
Using Literacy Resources in your community
17. 17
18. 18 Feasibility Testing in Process 8 practices (pediatrics, family medicine, internal medicine)
Each practice performs an assessment
Each practice chooses 5 tools to try to implement in 3 months
Follow-up phone calls to be completed end of September
19. 19 What are we learning? Practices start from very different levels
Health literacy expertise
Practice change expertise
Need to grab the attention of practices
Video helps
Get entire practice involved (not just clinicians)
Assessment results helpful
Practices want
�real life� examples
Quick start guide
Volume of tools is a bit overwhelming
Must be easy to navigate the toolkit
20. 20 Conclusion Conducted a thorough search for tools
Juxtaposed toolkit with chronic care model/medical home
Designed from perspective of making incremental changes
Overwhelming for some practices
Requires close attention and hard work, just like any reliable practice change
21. 21 Acknowledgements Authors
Darren DeWalt, MD, MPH
Leigh Callahan, PhD
Victoria Hawk, RD, MPH
Kimberly Broucksou, MSW, MPA
Ashley Hink, MPH
Rima Rudd, ScD
Cindy Brach, MPP Advisory Panel
Michael Barr, MD, MBA
Toni Cordell
Gail Neilsen, RTR, BSHCA, SAHRA
Michael Paasche-Orlow, MD, MPH
Ed Wagner, MD, MPH
North Carolina Network Consortium