Download
1 / 17
180 likes | 323 Views
Treatment and Secondary Prevention of Cancer-Associated Thrombosis. Supplement to Module 6. Overview. Introduction UFH as initial treatment for VTE LMWH as initial treatment for VTE Fondaparinux as initial treatment for VTE Transition to long-term therapy with vitamin K antagonists

E N D
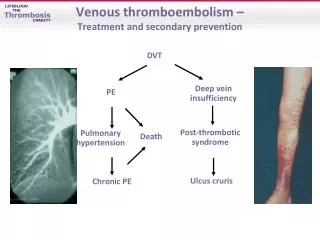
Treatment and Secondary Prevention of Cancer-Associated Thrombosis Supplement to Module 6
Overview • Introduction • UFH as initial treatment for VTE • LMWH as initial treatment for VTE • Fondaparinux as initial treatment for VTE • Transition to long-term therapy with vitamin K antagonists • LMWH as long-term therapy for secondary prevention of cancer-associated thrombosis
Goals of VTE Treatment • Prevention of fatal PE • Reduction of the morbidity associated with acute leg or lung thrombus • Prevention of recurrent VTE • Prevention of long-term sequelae
Initial Phase ≥5 d treatment with SC LMWH, IV UFH, monitored SC UFH, fixed-dose SC UFH, or SC fondaparinux1 Discontinue when INR >2.0 for 24 h Initiation of VKA together with LMWH, UFH, or fondaparinux on first treatment day Long-term Therapy Necessary for patients at continuous risk for recurrence Duration of treatment is dependent on underlying disease and risk factors Appropriate treatment can reduce the risk of recurrence to approximately 5% at 3 months2 Two Phases of VTE Treatment 1. Kearon C et al. Chest. 2008;133:454S-545S. 2. Prandoni P et al. Vasc Med. 1998;3:57-60.
Overview • Introduction • UFH as initial treatment for VTE • LMWH as initial treatment for VTE • Fondaparinux as initial treatment for VTE • Transition to long-term therapy with VKAs • LMWH as long-term therapy for secondary prevention of cancer-associated thrombosis
UFH as Initial Treatment for VTE • Traditionally, acute VTE has been managed with UFH, a parenterally administered agent with a rapid onset of action, followed by transition to oral anticoagulant • This paradigm became the gold standard following the landmark 1992 Brandjes study • Randomized patients with proximal-vein thrombosis to intravenous UFH plus acenocoumarol or acenocoumarol alone • Terminated early due to excess symptomatic events with oral anticoagulation alone (20%) compared with combination (6.7%) • Asymptomatic extension of VTE was seen in 39.6% of oral anticoagulant patients compared with only 8.2% of those who received combination Brandjes DP et al. N Engl J Med. 1992;327:1485-1489.
Limitations of UFH • Heparin is prone to nonspecific binding to proteins and cells • Poorly bioavailable at low doses • Marked variability in its anticoagulant response • Heparin has a relatively short half-life • Requires monitoring • Narrow therapeutic window • Associated with an increased risk for HIT and osteoporosis • Heparin resistance Hirsh J et al. Chest. 1998;114:489S-510S.
Overview • Introduction • UFH as initial treatment for VTE • LMWH as initial treatment for VTE • Fondaparinux as initial treatment for VTE • Transition to long-term therapy with vitamin K antagonists • LMWH as long-term therapy for secondary prevention of cancer-associated thrombosis
LMWH vs UFH as Initial Treatment for VTE: Comparative Meta-Analyses Lee AYY. In: Khorana AA, Francis CW, eds: Cancer-associated thrombosis: New findings in translational science, prevention, and treatment. Informa Healthcare USA. 2008.
Overview • Introduction • UFH as initial treatment for VTE • LMWH as initial treatment for VTE • Fondaparinux as initial treatment for VTE • Transition to long-term therapy with vitamin K antagonists • LMWH as long-term therapy for secondary prevention of cancer-associated thrombosis
Fondaparinux as Initial Treatment for DVT Büller HR et al. Ann Intern Med. 2004;140:867-873.
Overview • Introduction • UFH as initial treatment for VTE • LMWH as initial treatment for VTE • Fondaparinux as initial treatment for VTE • Transition to long-term therapy with vitamin K antagonists • LMWH as long-term therapy for secondary prevention of cancer-associated thrombosis
Vitamin K Antagonists as Long-Term Therapy • Once the INR has reached target during combination therapy, heparin is stopped and warfarin is continued for remainder of treatment • Longer-term VKA therapy (6 months) is more effective than shorter-term treatment (6 weeks) in preventing VTE recurrence Schulman S et al. N Engl J Med. 1995;332:1661-1665.
Limitations of Vitamin K Antagonists in Patients With Cancer • Patients with cancer remain at considerable risk for recurrent events even while taking oral anticoagulation1 • Incidence of recurrent VTE in patients with cancer taking warfarin is ~21%, compared with only 6.8% in patients without cancer2 • The incidence of bleeding in patients with cancer taking warfarin is substantially higher (12.4%) compared with patients without cancer (4.9%)1 • Levels of anticoagulation can be unpredictable with oral agents as a result of malnutrition, vomiting, and/or liver dysfunction that may occur in patients with cancer1 • Surgery and potential for chemotherapy-associated thrombocytopenia may require interruption of treatment1 • Poor venous access can impede laboratory monitoring1 1. Lee AY et al. N Engl J Med. 2003;349:146-153. 2. Prandoni P et al. Blood. 2002;100:3484-3488.
Overview • Introduction • UFH as initial treatment for VTE • LMWH as initial treatment for VTE • Fondaparinux as initial treatment for VTE • Transition to long-term therapy with vitamin K antagonists • LMWH as long-term therapy for secondary prevention of cancer-associated thrombosis
LMWH as Long-Term Therapy in Patients With VTE • 3 months of secondary thromboprophylaxis with enoxaparin or warfarin • Treatment failure (major bleeding or recurrent VTE) occurred in 21.1% of warfarin patients and 10.5% of enoxaparin patients (P=.09) • In a time-to-event analysis, enoxaparin was superior to warfarin Meyer G et al. Arch Intern Med. 2002;162:1729-1735.
LMWH as Long-Term Therapy in Patients With VTE • 6 months of thromboprophylactic therapy with coumarin derivative or dalteparin • Primary end point • First episode of symptomatic, recurrent DVT, PE, or both • 52% reduction in risk for recurrent VTE over 6-month study period • Dalteparin was not associated with increased risk for major or any bleeding • No difference between 2 groups in mortality Lee AY et al. N Engl J Med. 2003;349:146-153.