Download

1 / 48
500 likes | 590 Views
Blood Conservation in the OR. www.bestbloodmanitoba.ca. The m OR e we stick together…….. The less they will Bleed …. Patient Blood Management. What does this mean to you? Are there ways you practice this already?. Service Goals.

E N D
Blood Conservation in the OR www.bestbloodmanitoba.ca July 13th 2016
The mORe we stick together…….. The less they will Bleed…. July 13th 2016
Patient Blood Management • What does this mean to you? • Are there ways you practice this already? July 13th 2016
Service Goals • To enhance patient care and patient satisfaction through blood & blood alternatives education. • To provide a process whereby patients are informed and appropriate alternatives are implemented. • To promote adherence to established transfusion medicine guidelines. • To decrease the demand on the blood supply.
What population of patients do we see? Consultation Service for Perioperative Blood Management
Patient Blood Management • Patient Blood Management (PBM) is the timely application of evidence-based medical and surgical concepts designed to maintain hemoglobin concentration, optimize hemostasis and minimize blood loss in an effort to improve patient outcomes. July 13th 2016
BMS Strategies Pre-Operative Post-Operative Peri-Operative • Regional anesthesia • Controlled hypo-tension • ANH • Normothermia • Cell Saver • Surgical technique / meticulous hemostasis • Volume replacement • Pharmacological agents to reduce or control bleeding • Restricitve phlebotomy • Optimum fluid and volume management • Restrictive phlebotomy • Iron • Eprex • Early detection • Evaluation and management of anemia • Iron • Eprex • Restrictive phlebotomy July 13th 2016
Pre-operative • EARLY DETECTION – screening blood work at least 4-6 weeks prior to surgery 2. EVALUATION – etiology of anemia needed in order to treat 3. MANAGEMENT – options may include: • Diet modification and patient education to support adherence to plan • Medication – oral or parenteral iron, ESA, vit B12, folic acid, tranexamic acid, OCP to control bleeding (pre-surgical with menorrhagia) • Referrals to other services, i.e., hematology, gastroenterologist July 13th 2016 cell
Oral Iron Therapy July 13th 2016
Parenteral Iron Iron Sucrose(Venofer) Usual dose 200-500 mg IV infused over 90 minutes. Scheduled every other day. WRHA Iron clinic staffed by BMS nurses Very unique program- we are one of very few programs across Canada that have dedicated clinical space to administer IV iron/erythropoeitin to our patients July 13th 2016
Erythropoietin Stimulating Agents in Elective Surgery • Eligibility: • Anemia without reversible cause, no exclusionsto ESA. • Hemoglobin <130 g/L • > 10% Transfusion risk. • Can use with FE alone Use: • Requires lead-up time of 4-6 weeks. • Oral iron supplement for maximal benefit. • Doses individually assessed • Expected response is increase in HGB of 10-20 g/L & high reticulocyte count July 13th 2016
Preoperative Autologous Donation (PAD) • Refers to the donation of blood by a patient for their own use in scheduled elective surgery • Few good quality randomized controlled trials to highlight the benefits of PAD • Discard rates are above 50% for PAD- there is no crossover of these units into the allogeneic system when unused by the patient • Donation process can result in donor complications at a rate reported as high as 12 times greater than with healthy volunteers • PAD will be considered as a blood conservation strategy used by clinicians in Canada for selected patients only. These patients will have rare blood cell antigen types or unusual plasma protein deficiencies autologous donation with freezing of red cells for future use July 13th 2016
PAD Statistics 2009 – 2011 63 patients • Data on 43 patients • Units collected 77 • Units wasted pre-surgery 6 • Units available 71 • Units transfused 39 (55%) • Allogenicunits transfused 18 OR slates change, outdated Pre op anemia
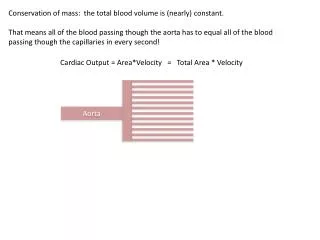
Perioperative Strategies • Regional anesthesia • Controlled hypotension • Normothermia • Cell Saver- (St.Boniface, HSC) • ANH- Acute Normovolemic Hemodilution (St.B, HSC) • Surgical technique/ meticulous hemostasis • Body Position • Anti-fibrinolytics July 13th 2016
Temperature Peri-operative hypothermia pre-disposes surgical patients to: • Bleeding • As little as 0.5 degrees below normal may increase blood loss by one unit of blood • Infection • 1.9 degrees cooler may increase risk of wound infection by 19% Anesthetized patients have an impaired ability to respond to hypothermia that lasts for several hours post-op… we must prevent hypothermia as a first line of defense. July 13th 2016
Cell Salvage July 13th 2016
Body Positioning in the OR • Circulatory modifications induced by perioperative positioning can be increased or decreased by anesthetic techniques. They will promote or oppose venous drainage in the surgical field. The aim is to decrease blood loss on the surgical zone concerned by bleeding. July 13th 2016
Tranexamic Acid • Evidence supports the routine use of TXA (Tranexamic acid) in hip and knee Arthroplasties to decrease intra and post-operative blood loss ( patient outcomes and adverse events considered) • Economic evaluations support routine TXA as cost savings • How does this help control bleeding? When a patient who is bleeding sometimes the blood clot is broken down too fast, which does not allow the body to stop and the wound to heal. Tranexamic acid works by blocking the breakdown of clots in the body. • CADTH-Prophylactic Tranexamic Acid Administration for Patients Undergoing Hip and Knee Replacement July 13th 2016
Fluid balance • Appropriate fluid resuscitation peri/post operative & maintaining adequate perfusion pressure. • Dehydration + low HGB = MORE dizziness & hypotension. Fluid boluses help pt to tolerate lower hgb levels. Assess for dehydration. • Encourage oral fluid intake after IV discontinued & prompt treatment/prevention of PONV to prevent fluid losses. July 13th 2016
Have we eliminated the risk of a blood transfusion? • The quality of blood that is issued is safer than it has been in the past. • However the risk in administering blood and the possibility of having a transfusion reaction still exists. July 13th 2016
Did You Know? Mislabeling tubes is the number one reason for near miss or possible transfusion reactions July 13th 2016
Label Blood Tubes Correctly • Major tertiray care center in Winnipeg had 43 occurences and 13 near misses in 2014 just in wrong labeled CBS blood tubes alone!!! July 13th 2016
In this example, incorrect labeling to the Pre-Transfusion Testing Tube put this cohort at risk for a Transfusion Reaction and additional blood loss due to need for repeat blood draws. In addition, 13 units of Blood Product were wasted for a total cost of approx. $6,500 July 13th 2016
Incorrectly labeled tubes is still the highest reason for a potential transfusion reaction in 2015. • New guidelines as of April 4th 2016 for all patients who have no sample in Trace Line to now have 2 samples sent. All patients who are identified as having no ABO will receive Group O specific blood until a second sample is sent or they receive 2 units of blood and are requiring more. • This has already prevented 2 potential transfusion reactions atWomen’s hospital. July 13th 2016
Created a poster series for clinicians that highlights the most pertinent steps to safer transfusion practices July 13th 2016
When do you Transfuse?? July 13th 2016
Perioperative Guidelines: Suggested Transfusion Trigger July 13th 2016 1 Perioperative Transfusion Medicine, Chapter 3
Actions for Nurses • Informed consent required (risks, benefits & available alternatives) More than a number! • Evidence based practice recommends that in stable, non-bleeding patients, often a single unit of blood is adequate to relieve patient symptoms and raise Hgb to an acceptable level. July 13th 2016
Preventing waste in the hospital • Minimal blood sampling & losses. (Use of Vamp systems in ICU, discontinue art/venous cath if not needed) • Small volume tubes & testing methods • Correctly label blood tubes- prevent blood letting • Intaoperatively- surgical hemostasis, use of antifibrinolytics & DDAVP when appropriate. -Cell salvage intraop - regional anesthetic • Prevention of hypothermia & hypovolemia postoperatively which can lead to coagulopathy. July 13th 2016
Education on appropriate transfusions • Ensure patient is normovolemic. Fluid bolus for hypotension & dizziness. Low hgb & dehydration= low B/P & dizziness. • Order one unit at a time in nonbleeding, stable patient. • Keep post-op patients warm. Temperatures below 36.0 cause coagulopathy & increased bleeding. • Anemia tolerance- generally healthy patients can tolerate lower hgb levels. July 13th 2016
How Successful has Blood Management Been? July 13th 2016
Success!! July 13th 2016
Where can you find resources?? • Past presentations on interesting blood topics • Transfusion Medicine Best Practice Manual July 13th 2016
Any Questions?? July 13th 2016


![[PDF] Blood Meridian: Or the Evening Redness in the West](https://cdn7.slideserve.com/12556520/slide1-dt.jpg)