Download
1 / 30
300 likes | 334 Views
Learn about spontaneous preterm abortion, causes, classifications, and treatment methods for early and late spontaneous abortions. Explore conservative and surgical management options to handle various scenarios.

E N D
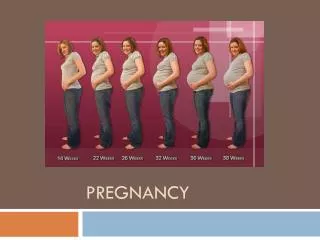
Pregnancy interrupting – spontaneous preterm interrupting of pregnancy: To 12 weeks of pregnancy – early spontaneous abortion 13-22 weeks – late spontaneous abortion 22-36+6 days– preterm labor
Causes of spontaneous abortions • Maternal • Infections – Listeria, Mycoplasma hominis, Ureaplasma urealyticum, Toxoplasmosis,Rubella, Cytomegalovirus. • Endocrine factors - luteal phase inadequacy, HyperthyroidismDiabetes Mellitus • Environmental factors • Uterine abnormalities 2. Paternal - chromosomal abnormality in either parent. 3. Fetal - genetic abnormalities of the conceptus, approximately half of which are autosomal trisomies.
Classification of abortions • Spontaneous • Induced Clinically: • Threatened • Initial • Inevitable • Completed • Incomplete • Missed
Threatened abortion Signs – lover abdominal pain. In bimanual examination – cervix is closed, enlargement of the uterus corresponds with gestational period Management – conservative.
Initial abortion Signs – lover abdominal pain, bloody vaginal discharge. In bimanual examination – cervix is closed, enlargement of the uterus corresponds with gestational period Management – conservative.
Inevitable abortion Signs – cramp abdominal pain thanks to uterine contractions, bloody vaginal discharge till profuse hemorrhage. In bimanual examination – cervix is dilated, products of conception are presented on cervical channel, enlargement of the uterus doesn’t correspond with gestational period – smaller Management –surgical – uterine curettage.
Incomplete abortion – retention of some conceptus inside the uterus Signs – lover abdominal pain, bloody vaginal discharge. In bimanual examination – cervix is dilated, enlargement of the uterus doesn’t correspond with gestational period – smaller, some products of conception should be expelled out. Management–uterine curettage
Complete abortion – all products of conception are expelled out of uterus Signs - lover abdominal pain, bloody vaginal discharge. In bimanual examination – cervix is dilated or closed, enlargement of the uterus doesn’t correspond with gestational period – smaller. Management–uterine curettage
Conservative treatment in the case of threatened and initial abortion • Bed rest • Sedative drugs • Spasmolitics – No-Spani, Papaverini hydrochloride • Analgetics – Analgin, Baralgin • Progesterone – Utrogestan, Duphastone,Endomerin • Chorionic Gonadotropin Hormone • Vitamines – vit. E • Hemostatics – Tranexamic acid
Stages of uterine curettage Anesthesia - paracervical block or general. • Bimanual examination • Disinfection of perineal region • Speculum insertion • Grasping the cervix for anterior lip with a toothed tenaculum. • Uterine probing- to identify the status of the internal os and to confirm uterine size and position. • Dilation of the cervix by Hehar’s dilators • Uterine curettage by sharp curette
Bed rest Sedative drugs – Valeriannae, Persen, Novopaside. Tokolotic agents: Magnesii sulfatis 40 ml 25 % in 400 ml isotonic solution, b2- adrenomimetics (2 ml ginipral in 500 ml isotonic solution). Progesterone – Utrogestan – 100 mg twice a day, Duphastone – 10 mg 2-3 times a day, Endometrin Spasmolitics – No-Spani, Papaverini hydrochloride Conservative treatment in the case of threatened and initial abortion in late terms (after 16 weeks)
Premature effacement (shortening of the vaginal portion of the cervix and thinning of the walls) and dilation of the cervix The dilation results in the amniotic membranes bulging through the opening and eventually rupturing, often before the baby can survive outside of the uterus. This irritates the uterus and brings on pregnancy interrupting. Cervical incompetence
Diagnosis is made by: medical history, physical exam, and ultrasound study. Diagnosis of Cervical Incompetence
Funneling of the cervix with the changes in forms T, Y, V, U (correlation between the length of the cervix and the changes in the cervical internal os). Cervix length < 25 mm Internal cervical os more than 10 mm Protrusion of the membranes. Presence of fetal parts in the cervix or vagina. Ultrasound findings
Funneling of the cervix with the changes in forms T, Y, V, U
A Shirodkar suture using Merselene tape at the level of the internal os is the treatment available.
McDonald suture with #4 mersilk at the level of the internal os
Preterm labor - is the term used to define infants who are born between22 and 36+6 weeks of gestation with the weight 500 – 2500 gram and length 25 - 47 cm
Threatened preterm labor Initial preterm labor Inevitable preterm labor Classification
Signs and Symptoms of Preterm Labor Threatened preterm labor is characterized by: • symptoms of pelvic pressure, low back pain; • increase uterine tone; • absence of cervical effacement and dilation in vaginal examination. Initial preterm labor is characterized by: • irregular crampy – like painful uterine contractions; • presence of cervical effacement and dilation of the cervix till 3-4 cm in vaginal examination; • amniotic fluid gush is present very often. Inevitable preterm labor is characterized by: • regular uterine contractions; • cervical dilation more than 3-4 cm.
1. Expectant Management - nonintervention or expectant management, in which nothing is done and spontaneous labor is simply awaited 2. Active Management - intervention that may include corticosteroids, given with or without tocolytic agents to arrest preterm labor in order that the corticosteroids have sufficient time to induce fetal maturation. Management of preterm labor
threatened and initial preterm labor; intact membranes; gestational age of pregnancy till 36 weeks of gestation; satisfactory maternal and fetal conditions; cervical dilation till 2-4 cm; absence of infection, regular uterine contractions, serious obstetric and extragenital pathology. 28-34 weeks of pregnancy with preterm ruptured membranes, absence of regular uterine contractions and infection. 28-34 weeks of gestation, intact membranes, 100 % cervical effacement and cervical dilation till 3-4 cm. Indications for expectant management:
1. Ultrasound examination is performed to help confirm gestational age, and assess amniotic fluid volume. Continuous fetal heart rate General blood analysis – twice a day determination of leucocytes number, urine, vaginal smear, bacteriological examination once a 5 days. 2. To 34 weeks of pregnancy for 24-48 hours Inhibiting preterm labor drugs are prescribed: 3. From 24-to 34 weeks: Accelerated Maturation of Pulmonary Function – 4. Group B-streptococcal infection prevention is recommended: Ampicillin 2g i/v initial dose than 1g i/v every 4 hours till delivery,or Cefazolin 2g i/v initial dose than 1g i/v every 8 hours till delivery,or Erythtomycin 500 mg i/v every 4 hours till delivery Expectant Management of Preterm labor in the case of Ruptured amniotic membranes:
Indications for active management: • preterm ruptured membranes; • regular uterine contractions; • presence of infection; • fetal jeopardy, hypoxia; • severe maternal diseases; • birth defects of the fetus; • obstetric complications of pregnancy (severe pregnancy induced hypertension, polyhydramnios). Vaginal delivery is indicated in cephalic presentations, cesarean section is performed in the case of breech presentation and transverse lie.
For tokolysis: - b-adrenergic inhibitors 2 ml Ginipral is dissolved in 500 ml isotonic solution with the rate 10 drops per minute, Niphedipine 10 mg every 15 min – 40 mg Magnesium sulfate – 20 ml 0.25 %in 200 ml isotonic solution Expectant Management of Preterm labor in the case of Intact amniotic membranes:
betamethasone (12 mg intramuscularly in two doses 24 hours apart) to prevent respiratory distress in the subsequently delivered preterm infant. dexamethasone, 6 mg intramuscularly every 12 hours - 24 mg all dose between 22 and 34 weeks. Repeated dose of hormones is not indicated. Accelerated Maturation of Pulmonary Function
Labor. Whether labor is induced or spontaneous, abnormalities of fetal heart rate and uterine contractions should be sought, preferably by continuous electronic monitoring. Delivery. Perineal protective maneuvers don’t apply. Intrapartum Management
Prevention of pregnancy interrupting in high risk patients !