Download
1 / 26
260 likes | 328 Views
Learn about the differential diagnosis, treatment options, and rehabilitation techniques for frozen shoulder, including stages of the condition and therapeutic interventions. Discover strategies for managing other capsular lesions and common shoulder ailments. Explore Neer classification, sub-acromial bursitis, and treatment approaches for various shoulder conditions.

E N D
The Shoulder Differential Diagnosis, Treatment and Rehabilitation
Capsular LR>ABD>MR
Frozen Shoulder • Aka Capsulitis or adhesive capsulitis • Vol of normal = 30mls • Vol of frozen = 3mls • 2% of normal population • 20% go bilateral • 11% in diabetic pop (don’t know why) • W:M 60:40 Non dom gtr than dom • Risk factors – diabetes, hyperthyroid, immobilisation, stroke
Frozen Shoulder • Capsular pattern Most loss of LR, then abd, then MR • Insidious onset • Self limiting 2-3 years • 3 Stages – freezing, frozen and thawing
Stage 1 • Intermittent ache • Not below the elbow • Able to sleep on that side • Elastic end feel
Stage 2 • Constant pain • Below the elbow • Unable to lie on that side at night • Hard end feel
Stage 3 • As in stage 1 • Resolving problem
Treatment of frozen shoulders • Stage 1 – heat, gentle mobilisation grade A and or injection • Stretch into elev and release with distraction • Distraction with sh elev and longitudinal distraction
Treatment of frozen shoulders cont. • Stage 2 – injection combined with pain relief (and slow sustained stretching, as able) • Stage 3 – heat + low load sustained stretching – LR, MR and elev • 20 – 30 mins
Other Capsular Lesions • OA • Electro and Grade B mobs • Steroid Sensitive Arthritis • Intra-artic injection
Primary impingement • Associated with anatomical changes in the sub-acromial space ? cause • Acromial shape • Osteophytes • Tendon changes – tendonitis Or tendinosis? • Ligamentous thickening • Bursal thickening
Secondary Impingement • Posture, neck and thorax • Tight muscle eg. Upper trapezius, pectoralis minor • Weak muscles eg.lower trapezius, serratus anterior • Poor timing, proprioception
Neer classification • Stage 1 – under 25 years, oedema, inflammation, acute bursitis, tendonitis • Stage 2 – 25-40 years, fibrosis, bursal thickening, fibre disruption in the tendons • Stage 3 – over 40 years, bony spurs, compromised space, partial to full thickness tears
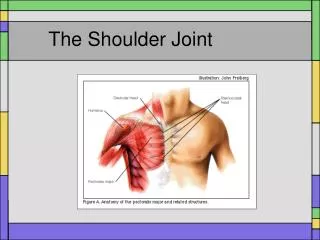
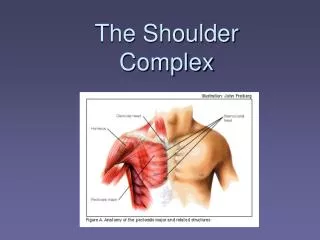
Sub-acromial bursitis • Aka sub-deltoid bursitis, SIS • Sub-acromial space – supraspin. Tendon, bursa, sup aspect of GH capsule and long head of biceps
On examination • Overuse • Gradual onset • C5 pain not usually below elbow • Arc and pain EOR • Non capsular pattern • Resisted abd and LR painful esp on release
Treatment of Subacromial Bursitis • Pain relief • Physio modalities eg acup, trig point, US, taping • Injection • Posture • Postural stability work inc lower traps • Rotator cuff strengthening • Stretching upper traps, pec major, minor
Acromio-clavicular Joint • O/E high painful arc • Localised pain C4 • Scarf positive • EOR pain on passive movements • Traumatic onset – RICE • Strapping • Mobs • Gradual onset -mobs, frics and or inject
Contractile Lesions • Strong + Painless = Normal • Strong + Painful = tendon or muscle local lesion I or II • Weak + Painless = Rupture III or nerve damage • Weak + Painful = severe lesion eg # • Pain during contraction – tendon • Pain on release - bursa
Supraspinatus Tendinitis • O/E resisted abd painful and painful arc = distal end of tendon • Friction + electro + rest • All frics numb + 10mins • Or inject • Resisted abd painful and no painful arc = MT junction • Rotation Friction with arm in horizon abd, no injec
Subscapularis Tendinitis • O/E resisted MR painful + painful arc = upper fibres + scarf test = lower fibres Friction – may be painful due to bursa Or inject
Infraspinatus Tendinitis • O/E resisted LR painful + painful arc = distal end of tendon + no painful arc = body of tendon • Friction or inject
Biceps Tendinitis • O/E resisted flexion and supination of the elbow painful • Long Head – rotation frics at bicipital groove or inject • Belly – pinch grip frics or inject with LA only
When its not a shoulder • Pins and needles / numbness • Radiation to hand • Neck movt aggravates pain • Gastro– intestinal pathology • Avascular necrosis