Download
1 / 44
470 likes | 920 Views
Basal Ganglia and Parkinson’s Disease. Talene Yacoubian, M.D., Ph.D. February 18, 2009. Overview. Basal ganglia terminology Basal ganglia anatomy Basal ganglia function and circuitry Disorders of the basal ganglia. what are the basal ganglia?. gray matter structures deep to the cortex

E N D
Basal Ganglia and Parkinson’s Disease Talene Yacoubian, M.D., Ph.D. February 18, 2009
Overview • Basal ganglia terminology • Basal ganglia anatomy • Basal ganglia function and circuitry • Disorders of the basal ganglia
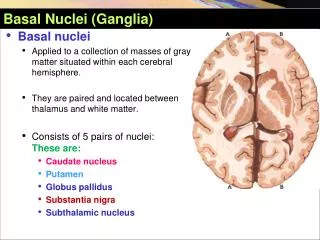
what are the basal ganglia? • gray matter structures deep to the cortex • comprised of several nuclei caudate putamen globus pallidus substantia nigra subthalamic nucleus nucleus accumbens
Basal ganglia nomenclature • striatum = caudate + putamen • “striped” body • lenticular nucleus = putamen + globus pallidus • “lens-shaped” • also known as lentiform nucleus • globus pallidus divided into two regions • externa and interna
Basal ganglia anatomy cingulate cortex caudate putamen internal capsule nucleus accumbens temporal cortex
Basal ganglia anatomy cingulate cortex internal capsule caudate globus pallidus externa putamen globus pallidus interna temporal cortex
Basal ganglia anatomy cingulate cortex internal capsule caudate globus pallidus externa putamen globus pallidus interna thalamic nuclei tail of caudate substantia nigra temporal cortex subthalamic nucleus
Basal ganglia functions • Modulation of movement • Initiate movement • Terminate movement • Role in cognition and learning • Role in emotional control
Basal ganglia connects to other brain areas • main input: cortex • main output: thalamus • multiple parallel pathways • these independent parallel pathways responsible for regulation of different functions cortex basal ganglia thalamus
Four major parallel pathways • motor loop • executive loop • limbic loop • eye movement loop
Inputs to basal ganglia • most of cortex projects to basal ganglia • only primary visual and auditory cortices do not • all inputs project to the striatum • putamen important in motor control pathways • receives input from premotor and motor cortices
Output of basal ganglia cortex • thalamus receives output in all loops • thalamic nuclei receiving output in motor loop: • ventral lateral nucleus (VL) • ventral anterior nucleus (VA) • output nuclei for motor loop: • globus palladus interna (GPi) • substantia nigra pars reticulata (SNr) • output projections are GABAergic • output projections inhibit thalamus striatum GPi/SNr VA/VL
Basal ganglia circuitry • two circuits important in regulation of movement • direct pathway • indirect pathway • direct pathway decreases inhibitory basal ganglia output • indirect pathway increases inhibitory basal ganglia output • balance of these two circuits underlies regulation of movements cortex putamen VA/VL GPe GPi/SNr STN
Direct pathway cortex putamen VA/VL GPe Glutamate (+) GABA (-) GPi/SNr STN
Direct pathway • Activation of direct pathway reduces inhibitory output of basal ganglia • Consequence is to promote movement
Indirect pathway cortex putamen Glutamate (+) GABA (-) VA/VL GPe GPi/SNr STN
Indirect pathway • Activation of indirect pathway increases inhibitory output of basal ganglia • Consequence is inhibition of movement
SN’s effects on direct and indirect pathways cortex putamen SNpc VA/VL GPe Glutamate (+) GABA (-) GPi/SNr STN
Dopamine’s effects on direct and indirect pathways • Dopamine release by SNpc activates direct pathway via D1 receptor • Dopamine release by SNpc inhibits indirect pathway via D2 receptor • Dopamine promotes movement
Basal ganglia circuits • Disruptions of motor circuits predict motor dysfunction • Parkinson’s disease as classic hypokinetic disorder • Huntington’s disease as classic hyperkinetic disorder
Case 1 • 65yo male presents with tremor in right hand. He reports that his handwriting has become less legible and small. He also notes that he has difficulty with buttons. His wife notes that when he walks his right arm doesn’t swing much.
Parkinson’s disease • hypokinetic disorder marked by loss of dopaminergic neurons in the substantia nigra • affects about 1% of population • prevalence expected to double by 2030 substantia nigra Parkinson’s disease normal
rest tremor bradykinesia/akinesia (slowness/ lack of movement) rigidity gait imbalance masked facies autonomic dysfunction orthostatic hypotension constipation sexual dysfunction cognitive impairment sleep disorders depression/anxiety Clinical features of Parkinson’s disease Motor features Non-motor features
Pathology of Parkinson’s disease PD normal • loss of dopaminergic neurons in substantia nigra pars compacta • classic pathological feature is Lewy bodies • cytoplasmic inclusions that stain for protein alpha-synuclein • more recently recognized that other brain areas involved Lewy bodies
Unknown in most cases! About 5% have clear genetic basis A-syn, parkin, DJ-1, LRRK2, PINK1 Potential pathogenic mechanisms: oxidative stress mitochondrial dysfunction protein misfolding inflammation Risk factors: Age Gender ?exposure to pesticides ?exposure to heavy metals History of head trauma Protective factors Caffeine Smoking High urate levels Etiology of Parkinson’s disease
Function of nigral dopamine neurons • dopaminergic neurons project to striatum • those that project to striatal neurons in direct pathway are excitatory (D1) • those that project to striatal neurons in indirect pathway are inhibitory (D2) • dopamine release by nigral neurons promotes movement
Nigral loss results in less movement cortex putamen SNpc VA/VL GPe Glutamate (+) GABA (-) GPi/SNr STN
Consequence of loss of substantia nigra • Loss of dopamine input: • Less activity of direct pathway • More activity of indirect pathway • Result: decreased movement
Treatment of Parkinson’s disease • Most current therapies are based on augmentation of dopamine levels or function • L-dopa • Dopamine receptor agonists • Monoamine oxidase inhibitors • COMT inhibitors
Dopamine neurochemistry DA D2R MAO COMT TH AADC tyrosine l-dopa dopamine DOPAC 3MT COMT MAO D2R HVA TH = tyrosine hydroxylase AADC = aromatic amino acid decarboxylase MAO = monoamine oxidase COMT =catechol-o-methyltransferase
Dopaminergic-based therapies from Singh et al. 2007
Limitations of current therapies • treatments are symptomatic • no clear evidence that disease progression is slowed • development of disabling motor fluctuations and dyskinesias • failure to treat non-motor symptoms
Case 2 • 46yo female teacher reports decrease in attention and difficulty planning lesson plans for class. Her family reports that she has become more irritable and has made hostile remarks to family members. She sleeps poorly and paces at night. They also note irregular movements in her arms that the patient tries to incorporate into purposeful movements.
Clinical features of Huntington’s disease • Autosomal dominant disorder • Secondary to expansion of CAG repeat in gene huntingtin • Marked by • Chorea: involuntary, writhing movements • Cognitive impairment and dementia • Psychiatric disorders
Huntington’s disease pathology • Preferential loss of caudate neurons that participate in indirect pathway • Result is excess movement (hyperkinetic)
Loss of caudate promotes movement cortex putamen VA/VL GPe Glutamate (+) GABA (-) GPi/SNr STN
Treatment • Currently no effective therapy for HD • Anti-dopaminergic drugs used to control chorea • dopamine receptor antagonists • tetrabenazine (dopamine depleter – inhibits dopamine transporter)
Summary • Basal ganglia comprised of several nuclei that regulate movement • Striatum is input center for basal ganglia • Balance of direct and indirect pathways underlies coordination of complex movements • PD is representative hypokinetic disorder • HD is representative hyperkinetic disorder