Download
1 / 46
460 likes | 636 Views
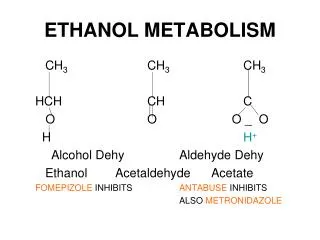
Methanol Blood Level Guidelines that Trigger Dialysis/Ethanol Therapy: What is the Evidence?. Mark Yarema, MD FRCPC May 2, 2002. Presentation Description.

E N D
Methanol Blood Level Guidelines that Trigger Dialysis/Ethanol Therapy: What is the Evidence? Mark Yarema, MD FRCPC May 2, 2002
Presentation Description The purpose of this presentation is to critically evaluate the current recommendations for the use of intravenous ethanol and hemodialysis in the treatment of methanol poisoning.
Case presentations Current recommendations for ethanol therapy and dialysis Calgary ‘protocol’ Literature review Remarks and conclusions Suggestions for future research Outline
42 year old man drinking paint thinner (unknown amount) developed abdominal pain to ED seen by Emergency Physician about 3 hours after ingestion no visual complaints methanol level 25 mg/dl (8 mmol/L), no acidosis Case #1
poison centre consulted, recommended IV ethanol and hemodialysis nephrology consulted, recommended IV ethanol with no hemodialysis discussion ensued between MD’s patient eventually started on IV ethanol and dialyzed for 4 hours. Repeat methanol level 6.3 mg/dl (2 mmol/L). Treatment stopped discharged from ED asymptomatic Case #1
38 year old man 4d Hx frontal headache admits to drinking etOH only no other symptoms meds = Tylenol #3 vitals N, exam N Case #2
Case #2 142 105 3.6 25 Glucose 4.2 BUN 2.7 ABG on r/a: 7.46 / 33 / 73 / 23 Measured osmolality = 333 mmol/kg etOH 13.3, acetone 12, isopropyl alcohol 4, ethylene glycol 0, methanol 8
started on IV etOH (10 cc/kg bolus then 1.95 cc/kg/hr) dialysis offered by nephro but refused by patient admitted to hospital on etOH drip on etOH drip for 70.5 hours, no acidosis, no visual symptoms. MeOH level < 3 discharged Case #2
The Question What should the blood methanol level be before initiating ethanol therapy and/or hemodialysis (HD) in patients without visual symptoms or metabolic acidosis?
Poisindex 2002“Ethanol therapy must be considered (with a) peak blood methanol level greater than 20 mg/dl (6.2 mmol/L)…continue ethanol until levels are below 10 mg/dl.” Ford 2001“Administer either fomepizole or ethanol until levels are measured below 20 mg/dl.” CurrentRecommendations
Ellenhorn 1997“start ethanol if peak methanol level is greater than 20 mg/dl...continue ethanol infusion until the methanol level falls below the range of 20 to 25 mg/dl” CurrentRecommendations
Poisindex 2002 “Indications for dialysis: Peak blood methanol concentration greater than 50 mg/dl (15.6 mmol/L)…” Rosen 2002“Hemodialysis is recommended by some authorities for a blood level of either substance greater than 25 mg/dl, whereas another authoritative consensus group advocates extracorporeal elimination for a level of 50 mg/dl” CurrentRecommendations
Ford 2001“Institute hemodialysis for a serum methanol level of 50 mg/dl or greater, regardless of symptoms or acid-base status…” Goldfrank 1998“Hemodialysis should be performed on any patient who has a blood level of methanol or ethylene glycol of 25 mg/dl…” Current Recommendations
Haddad 1998“Hemodialysis should be instituted if the blood methanol concentration is greater than 50 mg/dl and should be continued until the serum methanol level is reduced to the range of 25 mg/dl” CurrentRecommendations
varies depending on the case ethanol therapy initiated if methanol level > 6.2 mmol/L (20 mg/dl), or higher in some cases (repeat abusers) hemodialysis usually recommended once methanol level > 8 mmol/L (25 mg/dl) Calgary ‘Protocol’
literature reviewed for papers that provided blood level guidelines for ethanol therapy and/or hemodialysis in methanol poisoning review not meant to discuss indications for HD that are more easily agreed upon (visual symptoms, acidosis) Literature Review
Results: Ethanol therapy 2 articles Hemodialysis 5 articles Literature Review
Was assignment of patients randomized? Were all patients who entered the trial accounted for at its conclusion? Were patients and clinicians kept blinded as to which treatment was being received? Aside from experimental treatment, were groups treated equally? Critical Appraisal for Articles About Therapy
Were groups similar at start of trial? Was a number needed to treat calculated? Do these results apply to your patient? Are your patient’s values and preferences satisfied by the regimen and consequences? Critical Appraisal for Articles About Therapy
Swartz et al. Medicine 1981 case report of an outbreak of methanol poisoning in 46 patients 24 treated with ethanol in prison infirmary, 22 referred to tertiary care centre for ethanol +/- HD ethanol therapy continued until methanol levels were less than 30 mg/dl 6 patients developed visual sequelae, 3 patients died (all deaths were in those patients receiving HD) concluded that ethanol therapy should be continued until methanol levels are less than 20-30 mg/dl Literature Review
problems: small sample size limited data available in article no comment on return of symptoms after ethanol infusion stopped no comment on length of hospital stay treatment protocol not standardized unclear why 30 mg/dl chosen as criterion and why changed to 20-30 mg/dl in recommendations Literature Review
Ekins et al. West J Med, 1985 seven patients treated with ethanol and HD ethanol therapy commenced when methanol level greater than 20 mg/dl all patients dialyzed until methanol level < 20 mg/dl, then continued on ethanol until level < 20 mg/dl all patients survived, with only one having persistent visual disturbance concluded that ethanol therapy indicated when plasma levels are higher than 20 mg/dl (6.2 mmol/L) Literature Review
problems: small sample size average time spent on ethanol after HD was 18 hours (range: 0 - 70.5 hours) Literature Review
Cowen. Ann Int Med 1964 case report patient’s methanol level 360 mg/dl (112 mmol/L) on presentation started on ethanol therapy lost vision hemodialysis treatment stopped when methanol level 100 mg/dl (32 mmol/L) vision worsened Literature Review
dialysis repeated until methanol level 66 mg/dl (21 mmol/L), then stopped again treated with ethanol drip for 72 hours in hospital and subsequently discharged commented that “...ethanol can be used successfully to treat blood levels of 50 mg/dl or less. With higher levels…it would appear that hemodialysis is the only effective therapy.” Literature Review
Problems: case report care provided would not meet today’s standard statement of 50 mg/dl as indication for HD based on anecdotal experience Literature Review
Gonda et al. Am J Med 1978 May 9 patients treated with ethanol and hemodialysis dialysis continued for 4-6 hours, then ethanol therapy continued until methanol level undetectable 3 patients had permanent visual impairment, 2 died also reviewed all other published methanol overdoses to date (26 patients) recommended that hemodialysis be performed when methanol level > 50 mg/dl and continued until level is less than 25 mg/dl Literature Review
Problems: small sample size all patients had one of: methanol level well above 50 mg/dl acidosis visual abnormalities on presentation recommendation of HD until level < 25 mg/dl not practiced by study authors not enough information available to determine how long patients spent in hospital on ethanol after HD Literature Review Therefore, unclear why 50 mg/dl chosen as cutoff
Swartz et al. Medicine 1981 case report of an outbreak of methanol poisoning in 46 patients followed previous guidelines for HD (level > 50 mg/dl, severe acidosis) 13 patients dialyzed (no information available on length) 6 patients had persistent visual difficulties, 3 deaths concluded that dialysis may be useful to speed the elimination of methanol when blood levels are high, particularly over 100 mg/dl (32 mmol/L) Literature Review
Problems: small sample size limited data available in article unclear why 100 mg/dl chosen as cutoff impractical to treat patients with high methanol levels less than 100 mg/dl with ethanol therapy alone Literature Review
Becker et al. West J Med 1981 case report of methanol toxicity after consumption of 2 ounces of 20% methanol methanol level 140 mg/dl (45 mmol/L) ethanol therapy initiated and patient dialyzed for 6 hours with complete recovery commented that “methanol levels in excess of 50 mg/dl are probably an absolute indication for dialysis and ethanol treatment. When levels are below 50 mg/dl, ethanol treatment should be begun…” Literature Review
Problems: case report statement of 50 mg/dl as indication for HD not supported with evidence from case Literature Review
Jacobsen et al. Med Tox 1986 review article about all aspects of methanol poisoning reviewed literature as well as own unpublished cases commented that dialysis should be considered for patients with levels > 64.5 mg/dl (20 mmol/L), and that dialysis can be discontinued when levels are less than 32 mg/dl (10 mmol/L) Literature Review
Problems: recommendation made based upon unpublished data levels not advocated by other authors as indications for treatment Literature Review
the current recommendations are from case reports and retrospective case series textbooks often make conclusions on therapy without critically reviewing the evidence there is minimal data on safety of not treating peak blood methanol levels less than 20 mg/dl Remarks
levels of 25 and 50 mg/dl as criteria for HD not based on solid evidence (has evolved into more of a practical guideline) using level of 50 mg/dl will result in more people in hospital on ethanol infusions for longer periods of time using level of 25 mg/dl would decrease the amount of patients treated on ethanol infusions in hospital but would result in increased utilization of dialysis Remarks
better predictors of need for treatment and final outcome than methanol level: coma seizures pH < 7.0 increased formic acid levels Remarks
for ethanol therapy: current guidelines suggest initiating therapy when level > 20 mg/dl (6.2 mmol/L) limited information on safety of not treating patients with peak levels of < 20 mg/dl without acidosis or visual disturbances Summary
for hemodialysis: using a level of either 25 or 50 mg/dl as your criterion must be done with the knowledge that: the evidence to support either level is minimal (and in fact 25 mg/dl has never been studied) long half life of methanol while on ethanol requires prolonged stay in hospital methanol level itself is not a good predictor of outcome and should be interpreted with the entire clinical situation Summary
future research suggestions: effectiveness of fomepizole (now available in Canada) vs. ethanol in treatment of methanol poisoning clarification of lowest blood level of methanol that requires no therapy Summary