Download
1 / 32
660 likes | 3.71k Views
THE SACROILIAC JOINT. Anatomy Biomechanics Evaluation. SACROILIAC CLASSIFICATIONS. Diarthrodial Joint- Atypical Synovial with joint capsule present only on the anterior aspect Amphiarthrodial- Only displays 0-3˚ of movement- Avg. 0.2 ˚

E N D
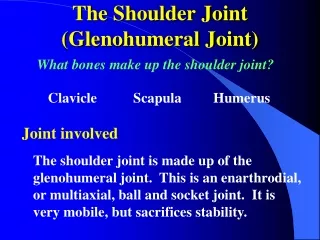
THE SACROILIAC JOINT Anatomy Biomechanics Evaluation
SACROILIAC CLASSIFICATIONS • Diarthrodial Joint- • Atypical Synovial with joint capsule present only on the anterior aspect • Amphiarthrodial- • Only displays 0-3˚ of movement- Avg. 0.2 ˚ • Many interlocking osseous structures limits gross excursion • Bound by strongest ligaments in the body • Basically, a case of semantics
Sacroiliac Pain and “Dysfunction” • Accommodation (Secondary) : • Structural anomalies- leg def, sacral • Muscle imbalance (function) leading to coronal imbalance and pelvic distortion • Superior subluxations • Hip, Knee, Ankle or Foot PAIN • Primary subluxation: • Direct trauma • Chronic subluxation (leads to OA) • Child birth
Why is it the least understood joint? Very difficult to scientifically analyze • Reliable tests need to be: • 3-dimensional • multiple titanium spheres into the bones or rigidly fixed external devices • In vivo- standing, prone, supine, hip movements COA- Moore
What Research Has Shown • The range of sacroiliac motion in any plane (transverse, longitudinal or AP axis) is less than 2˚, and usually less than 1˚ • Although the S/I jts move, their direction of movement is irregular • ROM is limited increasingly with age • Instability due to ligamentous sprain or pregnancy can also be a major cause of sacroiliac pain
UNLIKE ANY OTHER MAJOR JOINT IN THE BODY • It’s ranges of movement are very small • No muscles that execute active movements of the joint (mm that cross act on L-spine or lower extremity) • Structurally and functionally more like an intertarsal joint (passive movement) • STRESS-RELIEVING JOINT
SACRUM • Two Unique Roles: • Longitudinal direction: Supports L-spine • It’s hyaline cartilage is designed for transmitting forces to the pelvis • Transverse direction: Transmits force to the lower extremities • It’s fibrocartilage-like hyaline cartilage is designed to absorb forces
Sacral Anatomy • Size and shape of the human ear • Articular surface: • S1-S3 • Irregular contour • Major depression on S2 (receives Bonnaire’s tubercle) S, SC & ANS- Cramer & Darby
SACRUM • “Key Stone in an Arch” • Increased vertical load leads to an increase in joint surface bonding • No downward gliding under weight of the body • Sacrum is set obliquely between ilia, so under vertical loads, it nutates • Rotates around Bonnaire’s Tubercle.
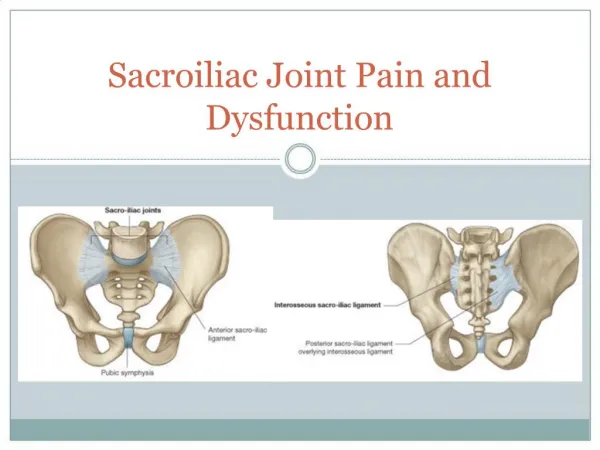
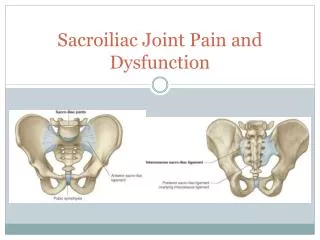
LIGAMENTS • Interosseous S/I Ligament- • Most important in the S/I joint and some of the toughest in body • Anterior Articular Capsule S, SC & ANS- Cramer & Darby
LIGAMENTS • Posterior S/I Ligament- • Long- Prevents counternutation • Short- Binds Ilia 4. Anterior S/I Ligament
Supporting Ligaments Associated with the S/I Joint Sacrospinous ligament Sacrotuberous ligament
BIOMECHANICS Of the Sacroiliac Joint
AGE CHANGES THINGS • 0-20 Smooth gliding planes • 20-50 Interlocking irregularities • >50 Hypomobility • >80 Osteophytic, Immobile
S A C R O I L I A C “How I Spell Relief” • If the pelvis were a solid ring of bone…. • The sacrum is placed strategically in the pelvic ring at the site of maximum torsional stress • Twisting forces are absorbed by the ligaments • Strong and Stable joint (bony locking mechanisms)
Sacroiliac Joint Motion Cycles of Alternating Flexion and Extension During Locomotion • S/I flex and extend in unison with hip joint: • Lower limb flexion: • Ilium (PSIS) goes PI, sacral base goes AI • Lower limb extension: • Ilium (PSIS) goes AS, sacral base goes PS • Rocking action between sacrum and ilium occurs as weight is imposed from one leg to the other
Sacroiliac Fixation • Most often a SYMPTOM rather than a PRIMARY cause of distortion • The total pelvis tips, sways and rotates in accommodation to eccentric weight imposition upon it: • Unequal weight into each S/I joint- leads to abnormal gait • Pelvis consistently responds to changes in weight distribution
Sacroiliac Fixation • Continued stress leads to: • Fixation • Sclerotic changes (OA) • Gross muscular compensation- holding joint in the fixed malposition
EVALUATION of the S/I JOINT • Challenging: • Wide range of normal anatomy • Cannot directly palpate the joint • Must rule-out deficiencies above and below the joint • Functional components are a major contributor to S/I pain
EVALUATION of the S/I JOINT • History • Negative Neurological Signs • Positive S/I jt. Orthopedic tests • Medical Diagnostics: X-ray guided injections of lidocaine
Common Reasons for S/I Joint Dysfunction or Pain • Osteoarthritis • Pregnancy • Leg deficiency • Lower extremity pain • Rule-out: • Pelvic disorders • Enteric disorders • Inflammatory arthrotides
EVALUATION of the S/I JOINT • Evaluated in all 5 postures: • Standing • Seated • Prone • Supine • Side posture
STANDING EVALUATION • Postural Analysis: Look for leg deficiency, or any structural asymmetry • Check for • Alignment • Tenderness • Mobility • Gillett's Analysis: • S2 and PSIS- Flexion and Extension • S4 and PIIS- Flexion and Extension • Belt Test
SEATED EVALUATION • Internal and External Rotation with approximation and flaring of thighs • Flexion-PI and Extension-SA
PRONE EVALUATION • Palpation- Bony landmarks, Soft tissue: TTT, Tone, Mobility—COMPARISON of both sides • PSIS • Lumbosacral joint • Iliac Crest • Sacroiliac ligaments • Gluteal mm • Iliolumbar ligaments
PRONE EVALUATION • Spring the S/I joints • Stabilize sacral base and extend lower limbs • Hip extensors • Hibbs (modified) • Yeoman’s (extension)
SUPINE EVALUATION • S/I Stretch Test- • Press laterally on ASISs with hands crossed (challenges anterior S/I) • Gaenslens (extension) • Hip abduction • Hip adduction • Hip flexion
SIDE POSTURE EVALUATION • Sacroiliac Resisted Abduction Test • Iliac Compression • Lewin-Gaenslen’s Test
LEG LENGTH CHECKS • Anatomical or functional discrepancies in leg length may predispose the patient to pelvic dysfunction • X-ray evaluation • External measurement • Functional leg length test • Use of the bilateral weight scales
LEG LENGTH CHECKS • TRADITIONAL CHECK • Patient is Prone • Observe comparative length of heels or medial malleoli • Flex knees to 90˚ to check for shortened tibia • Functional leg length inequality secondary to S/I subluxation may reverse from changing positions
SUMMARY • S/I joint does NOT move of its own accord, but rather accommodates to changes in weight bearing • S/I joint does NOT allow for gross excursion or slippage due to anatomical restrictions
Primary Subluxations are Due to: • Direct trauma- sprain • Chronic subluxations and muscular imbalance which leads to OA • Pregnancy