Download
1 / 22
220 likes | 267 Views
ACID – BASE DISORDERS. M. Tatár. H + affects structure and function of proteins. . changes of cellular enzymes activity. . cellular and organ functions changes. Sources of H + in organism. a) Volatile acid CO 2 + H 2 O H 2 CO 3 H + + HCO 3 -. b) fixed acids

E N D
ACID – BASE DISORDERS M. Tatár
H+affectsstructure and function of proteins changes of cellular enzymes activity cellular and organ functions changes
Sources of H+ in organism a) Volatileacid CO2 + H2O H2CO3 H+ + HCO3- b) fixedacids H2SO4, H3PO4 c) organicacids lacticacid, ketoacids
Hydrogen ion [ H+ ] = from 10 - 7,44 to 10 - 7,36 = 0,000000036 - 0,000000044 mol . l-1 = 36 - 44 nmol . l-1 pH = - log [ H+] mol . l-1 pH = 7,4 0,04 mitochondria : 2 - 5 active H+
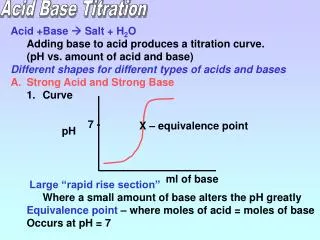
H+ (nmol.l-1) 160 140 120 100 80 acidaemia 60 norm 40 basaemia 20 pH 6,8 7,1 7,4 7,7 norm acidaemia basaemia
acidemia - acidosis alkalemia - alkalosis
HENDERSON – HASSELBALCH equation [ H+ ] . [ HCO3-] K = --------------------- [ H2CO3] [ H2CO3] [ H+ ] = K . ---------------- [ HCO3-] 1 1 [ HCO3-] log ----- = log ----- + log ------------- [ H+ ] K [ H2CO3] [ HCO3-] pH = pK + log ------------ [ H2CO3] 24 mmol pH = 6.1 + log ----------- ( log 20 ) 30/1.5 18/0.9 1.2 mmol pH = 6.1 + 1.3 = 7,4
Buffers 1 [ HCO3- ] 1. Bicarbonatesystem ------------ [ H2 CO3 ] HCl + NaHCO3 H2 CO3 + NaCl NaOH + H2 CO3 NaHCO3 + H2O Hb 2. Hemoglobinsystem--------- HbO2
Buffers 2 proteinate- 3. Plasmaproteins--------------- H - protein HPO42- 4.Phosphatesystem---------- H2PO4- HCO3- - 53% (plasma 35%, RBC- 18%) BuffersHb - HbO2 - 35% in bloodPhosphates - 5% Plasm. prot. - 7%
Proximaltubule „reabsorbed“ HCO3- Na,K,ATP-ase
Distalnephron „new“ HCO3-
13.3 10.6 hypoventilation 8.0 (kPa) 6.7 Pco2 5.3 4.0 hyperventilation 2.7 7.4 7.6 7.0 7.2 pH
Mechanisms of acid – base disorders metabolic metabolic 4. alkalosis 1. acidosis 2. alkalosis 3. acidosis HCO3- pH = pK + log ---------------------- PCO2 respiratory 5. acidosis 6. alkalosis
Anion gap [ Na+ ] - ( [Cl-] + [ HCO3-] ) = 10 - 12 mmol.l-1 140 - ( 104 + 24 ) = 12 mmol.l-1 > organic or fixed acids
Causes of metabolic acidosis (MAC) I.Normalaniongap MAC bicarbonate loss hyperchloremic MAC a) viathe GIT: diarrhea, smallbowel fistula b) renaltubularacidosis (reduced H+excretion) [ Na+ ] - ( [Cl-] + [ HCO3-] ) = 12 mmol.l-1 II. Highaniongap MAC gains of noncarbonic acids a) lactic acid: hypoxia, liver insufficiency b) ketoacidosis: diabetes mellitus, starvation c) retention of fixed acids: renal failure [ Na+ ] - ( [Cl-] + [ HCO3-] ) > 12 mmol.l-1 acids
Compensatory response in MAC 1. ventilation M M ----- ----- R R 2.HCO3- retentionin kidneys Clinical features - Kusmaulbreathing - cardiaccontractility - lethargy - renalosteodystrophy - hyperkalemia - vomiting
Causes of metabolic alkalosis (MAL) PrimaryCl-lost(hypochloremicalkalosis) b) kidneys: diuretics (furosemid) a) GIT: prolongedvomiting Cl- and HCO3-have a reciprocalrelationshipsto maintaineelectroneutrality of ECF [ Na+ ] - ( [Cl-] + [ HCO3-] ) = 12 mmol.l-1
Compensatory response in MAL 1.Alveolarhypoventilation M M ------ ------- R R 2.Renalexcretion of theexcess HCO3- Clinical features - occasionally tetany - risk of cardiac dysrhythmias - afinity of Hb to O2 - hypokalemia
Causes of respiratory acidosis (RAC) Respiratorydisorders CO2accumulation - alveolarhypoventilation Compensatory response HCO3- retentionin kidneys M M ------- ------- R R Clinical features - CNS dysfunction: confusion, somnolence - cerebral vasodilation: intracranial pressure
Causes of respiratory alkalosis (RAL) Alveolarhyperventilation - respiratory centre stimulation a)the most common: anxiety and emotional stress b)hypermetabolic conditions: fever, CNS lesions, thyreotoxicosis c)hypoxia: pneumonia, pulmonary edema, high altitude Compensatory response Clinical features renalexcretion of HCO3- M M ------ ------- R R - vomiting • tetany