Download

1 / 20
210 likes | 512 Views
Parotid gland – Anatomy & tumours. Parotid gland. Paired unilobular glands divided non anatomically by the facial nerve into deep and superficial lobes Accessory parotid tissue may extend along parotid duct into buccal space

E N D
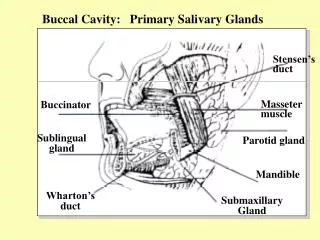
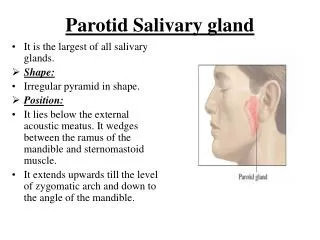
Parotid gland • Paired unilobular glands divided non anatomically by the facial nerve into deep and superficial lobes • Accessory parotid tissue may extend along parotid duct into buccal space • Pyramidal in shape and lies in pre auricular area, inferomedial to external auditory meatus • Posterior: mastoid and tympanic processes of temporal bone, external auditory canal and styloid process • Lateral: Parotid fascia, SMAS • Medial: Masseter • Superior: Zygomatic arch • Inferior: Sternocleidomastoid, posterior belly of digastric • Apex may extend low into neck along sternocleidomastoid, and postero-medial gland extends into retromandibular area through stylomastoid tunnel into parapharyngeal space
Supply of parotid gland • Blood supply is terminal branches of ECA, especially STA and internal maxillary artery • Venous drainage is to posterior facial vein • Sensation is via auriculotemporal branch of V3 and greater auricular nerve (C2,3) • Sympathetic supply from inferior (IX to otic ganglion, V3, auriculotemporal nerve) and superior salivatory nuclei (CN VII) • Parasympathetic supply from T1-2 via sympathetic chain and superior cervical sympathetic ganglion and arterial plexus • Parotid and preauricular lymph nodes receive drainage from upper half of face and scalp • Then onto jugulodigastric nodes of deep cervical chain
Parotid (Stensen’s) duct • Arises at anterior border of gland as confluence of several large ducts • Runs across lateral surface of masseter, closely accompanied by buccal branch of facial nerve • At anterior border of masseter, the duct pierces buccinator and enters the oral cavity opposite the second molar
Histology • Salivary glands are composed of serous and mucous acini, the proportions of which determine the type of salivary secretion from each duct • Parotid is mainly serous • Sublingual is mainly mucous • Submandibular is mixed • Minor salivary glands tend to be under local control, whereas major glands are parasympathetically controlled • Saliva is hypotonic, with low concentrations of NaCl, high KHCO3 • Antibodies (IgA), amylase, lysozyme. lactoperoxidase • Submandibular saliva has relatively high Ca • Main function is lubrication and cleansing oral cavity • Initiation of starch digestion • Immunological • HCO3 retards growth of acidophilic bacteria • Maintenance of dentition (Ca, Po4, Mg) • Normal outflow is 1-2L/day
Anatomy of facial nerve – Extratemporal • Exits stylomastoid foramen 1cm superior to mastoid process and 1cm deep to lateral surface • Indicated by tragal pointer (junction of cartilaginous paortion of EAM with skull), which is 5-6mm from stylomastoid foramen • Other method of finding facial nerve trunk is to follow the tympanomastoid fissure (junction of posterior bony auditory canal and mastoid portion of temporal bone) • Nerve lies 6-8mm below inferior end of this line • 3 branches given off just below stylomastoid foramen • Posterior auricular nerve (to postauricular and occipital muscles) • Nerve to stylohyoid • Nerve to posterior belly of digastric • Nerve runs lateral to styloid process and enters parotid gland between stylohyoid and digastric, lateral to external carotid artery and posterior facial vein • Lateral to EJV, CNVII branches into zygomaticotemporal and cervicofacial trunks (pes anserinus) • Usually within 2cm from exit of stylomastoid foramen and within 1cm of entering the parotid gland • Runs between deep and superficial lobes of parotid gland • Innervates muscles of facial expression from their deep surface; except mentalis, buccinator and levator anguli oris which all lie deep to CN VII • Nerve to muscle fibre ratio is 1:8 (normal muscle is 1:50)
Branches of facial nerve • Many variations • Temporal and marginal mandibular are most consistent • Pitanguy’s line • 6mm below EAM to 1-2cm above lateral brow is the extent of anterior branches • Usually 2-3 frontal branches in an area 1-3cm lateral to lateral canthus along zygomatic arch • Anterior to superficial temporal vessels and deep to SMAS layer • Buccal branch • Lies along line joining tragus to midline upper lip • Many connections between buccal and zygomatic branches in buccal fat pad • Marginal mandibular branch • Always lies superficial to facial vessels • Runs within 2.5cm inferior to mandible. Anterior division of cervical branch usually runs parallel and 1cm inferior
Tumours • WHO classification identifies 46 types of salivary gland tumours • 2 theories of development • Dedifferentiation – mature elements respond to oncogenic stimulus • Bicellular (Eversole) – neoplasms arise from stem or reserve cells • Majority of tumours arise in parotid gland, but tumours of minor salivary glands are more likely to be malignant (20% parotid, 50% submandibular, 70% minor) • Histological features and stage rather than site of origin are major determinants of outcome
Pleomorphic adenoma • Most common primary salivary tumour • Benign epithelial cells surrounded by myoepithelial cells interspersed with areas of myxoid or chondroid stroma • Proportions of cellular and myxoid stroma vary considerably and do not predict malignancy • Cell of origin is the reserve cell of intercalated ducts, which may differentiate into epithelial or myoepithelial cells • Usually present as a solitary painless mass • Most grow in the parotid gland and 70% parotid tumours are pleomorphic adenoma • Most grow in tail, but 10% involve the deep lobe • Slight F>M, tumour usually presents in 5th decade • Slow growing and encapsulated early • Can extend as pseudo pods beyond the tumour mass, which increases risk of local recurrence • Risk of malignant change is <10%, but increased in recurrences
Monomorphic adenoma • Benign neoplastic growths composed entirely of a single epithelial cell type • Epithelium forms a regular (usually glandular) pattern without mesenchymal tissue characteristics of pleomorphic adenoma • Most common subtypes are papillary cystadenoma lymphomatosum (Warthin’s tumour) and oxyphillic adenoma (Oncocytoma) • Arise from intercalated duct cell • Account for 4-8% salivary gland neoplasms • Propensity towards multicentricity • Have the capacity to transform into pleomorphic adenomas
Warthin’s tumour (Papillary cystadenoma lymphomatosum) • Most common monomorphic adenoma • Neoplastic duct epithelium and prominent lymphoid element • Accounts for 6-10% parotid tumours • May also occur in heterotopic salivary tissue • Occurs when lymphoid encapsulated epithelial tissue is subjected to an oncogenic stimulus • High incidence of multicentricity and bilaterality (10%) leading to high local recurrence • 5:1 M:F, > 90% are smokers • Usual presentation is asymptomatic mass in tail of parotid at angle of mandible
Mucoepidermoid carcinoma • Most common primary parotid gland malignancy, and second to adenoid cystic carcinoma in the other salivary glands • Most commonly occurs in 5th decade of life, but also most common salivary gland tumour in children • F:M = 2.4:1 • Arise from basal cells of the excretory duct system • Composed of mixed epidermoid and mucous secretory malignant cells
Adenoid cystic carcinoma • Most common malignant tumour of the submandibular, sublingual and minor salivary glands • Only 15% parotid gland cancers • Cell of origin is intercalated duct reserve cell • Also called cylindromas because of cribriform pattern, but histological appearance varies considerably • Tend to grow slowly and invade locally • Characterised by invasion beyond the palpable and visible mass • Perineural invasion is common • More commonly than any other tumour will present with pain and facial nerve paralysis
Metastatic carcinoma • May occur by lymphatic or haematogenous spread, contiguous extension • Contiguous spread is most commonly seen with locally invasive or advanced overlying tumours of the skin • Lymphatic spread can occur from anywhere in upper face/scalp, and occasionally deeper structures to deep lobe • SCC and melanoma are the most frequent tumours to metastasize to the parotid • Haematogenous metastatic carcinoma to the parotid most commonly arises from primary tumours in the lung, breast, kidney or GIT
Other tumours • SCC • True SCC parotid is only diagnosed after exclusion of metastatic SCC • Arises from basal cell of excretory duct • Strongly associated with tobacco use • High grade malignancy with perineural invasion, regional and distant metastatic disease and local recurrence • Lymphoma • Primary malignant lymphoma of salivary glands is rare, constituting 4-5% extranodal lymphoma • Typically patients in 6th -7th decades • Usually NHL, then diffuse large cell lymphoma