Download
1 / 20
250 likes | 637 Views
Parathyroid gland. M. Alhashash. Anatomy . Anatomy . Physiology . Parathyroid Imaging. Tc-99m sestamibi scan ( Cardiolyte ) Ultrasound Initially thought useful only in persistent or recurrent disease. Thallium-technetium subtraction scan - now rarely used.

E N D
Parathyroid gland M. Alhashash
Parathyroid Imaging • Tc-99m sestamibi scan (Cardiolyte) • Ultrasound • Initially thought useful only in persistent or recurrent disease. • Thallium-technetium subtraction scan - now rarely used
Parathyroid Imaging -Tc-99m Sestamibi 45 min Anterior 45 min LAO submandibular gland thyroid lobe adenoma Delayed views 2 HR 2 HR
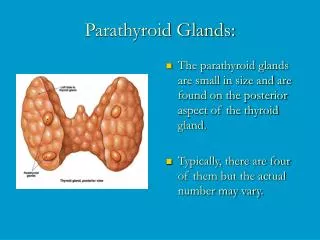
Disorders of Parathyroid Glands • Hypoparathyroidism-rare. Almost always caused by excessive surgical removal of parathyroid tissue (iatrogenic) during thyroid or parathyroid surgery • Hyperparathyroidism (HPT): • primary - high Ca++, high PTH - usually due to single adenoma (90%), cured by removal of adenoma • secondary - low Ca++, high PTH, seen in chronic renal failure - not a surgical problem • tertiary - high Ca++, high PTH, seen after renal transplant - hyperplasia of all 4 glands
Primary hyperparathyroidism • The commonest. • Autonomous production of PTH. • Pathology: • Neoplasm(85%). • Adenoma (80%) usually single gland • Carcinoma (5%) usually associated with hyperplasia or adenoma. • Hyperplasia(15%)usually 4 glands and may be associated with MEN syndrome.
Primary hyperparathyroidism • Clinically: • Females > males • Symptoms of hypercalcaemia. • Abdomen: anorexia, nausia, vomiting, hypotonia---peptic ulcer---pancreatitis. • Renal: stones , polyuria , nephrocalcinosis, renal failure, hypertension. • Skeletal: intense bone resorption, pathological fractures, calcification of cartilages and pain. • Psychotic: apathy, drowsiness and depression. • General : weakness, pruritis, neuropathy, numbness, thirst, salivary gland calculi. • Hypercalcaemic crisis: Ca > 15mg % confusion and coma.
Investigations • Hypercalcaemia (normal Ca 9.2 – 10.4mg%). • Hypophosphataemia. • PTH • Plain x-ray bone and stones • U/S, CT , MRI, • Isotope scanning
Treatment • Hyperplasia subtotal parathyroidectomy. • Adenoma resection of the affected gand/s. • Carcinoma: hemithyroidectomy with the gland followed by radiotherapy. • Hypercalcaemic crisis : I.V. phosphate, calcitonin, saline and diuretics .
Secondary hyperparathyroidism. • In chronic renal failure - hypocalcaemia-hyperplasia of the gland. • Clinically : mainly bone resorption. • Treatment: mainly medical • Restriction of phosphate. • Calcium. • Vitamin D. • surgery only in severe cases by subtotal parathyroidectomy • Localization as primary.
Tertiary hyperparathyroidism • After renal transplantation • Sever bone manifestation. • Subtotal parathyroidectomy.
Traditional Surgery for Hyperparathyroidism • primary HPT - 4 gland exploration, remove adenoma, biopsy 3+ normal glands • tertiary HPT (after renal transplantation) - 3 1/2 gland removal +/- forearm autotransplant
Complications of Parathyroid Surgery • persistent HPT - 1-20% (experience dependent) • temporary or permanent hypocalcemia - 1-20% • nerve injury - recurrent or superior laryngeal -1-10% • bleeding - <5%
Unilateral Exploration for Primary HPT • if: one abnormal, hypercellular gland and one normal gland found on one side, no contralateral exploration • occasional use of preop thallium-technetium scan • results of 5 studies - cure 93-100%
Parathyroid gland Thank you