Download
1 / 34
550 likes | 3.44k Views
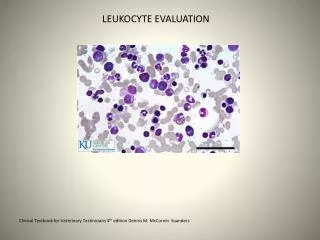
Morphologic and Distributive Leukocyte Disorders. LabM 321 Introduction to Clinical Hematology Winter 2010 ©Cara Calvo, MS, MT(ASCP)SH – UW, 2009 - 2010. Graphic accessed http://www.med-ed.virginia.edu/courses/path/innes/images/wcdjpeg/wcd%20dohle%20x100.jpeg , 2001. Introduction.

E N D
Morphologic and Distributive Leukocyte Disorders LabM 321 Introduction to Clinical Hematology Winter 2010 ©Cara Calvo, MS, MT(ASCP)SH – UW, 2009 - 2010. Graphic accessed http://www.med-ed.virginia.edu/courses/path/innes/images/wcdjpeg/wcd%20dohle%20x100.jpeg, 2001.
Introduction • Leukocytes function to protect the body against foreign organisms or antigens. • In doing so, they undergo visible changes that can be detected and evaluated macro- and microscopically. • The changes fall into two categories: • Quantitative or macro changes • alterations in numbers of cells • Absolute • Relative • Qualitative or micro changes • alterations in cell morphology • Nucleus • Cytoplasm Graphic accessed http://home13.inet.tele.dk/gloerud/yellow_l.gif, 2008.
DefinitionsWhite Cell Numbers • Leukocytosis: increase in the numbers of circulating white cells • >12,000/uL • Leukopenia: decrease in the numbers of circulating white cells • < 4,000/uL • Left Shift – increased circulating numbers of immature neutrophils • Leukoerythroblastic Reaction – leukocytosis with a left shift accompanied by nucleated red cells: seen in malignancy. • Leukemoid Reaction – benign excessive leukocytosis accompanied by an exaggerated neutrophilia and a left shift in response to an infection; the WBC > 50 x 109/L • Leukocyte Alkaline Phosphatase – stain used to differentiate a leukemoid from a leukoerythroblastic reaction Graphics accessed URL http://atlasgeneticsoncology.org/Anomalies/t0422q12q11ID1153.html & http://www.med-ed.virginia.edu/courses/path/innes/wcd/leukocytosis.cfm, , 2010. http://www.med-ed.virginia.edu/courses/path/innes/images/wcdjpeg/wcd%20leuko%20Eblastic%20x50.jpeg
Neutrophilia>7.5 x 109/L Other defining features: • Left shift • Increased band forms • “toxic” cell appearance • Dohle bodies • Vacuoles • Intra-cellular microbes Graphisc accessed http://www.accessmedicine.com/loadBinary.aspx?name=licha&filename=licha_II.B.001.jpg, and http://www.wadsworth.org/chemheme/heme/microscope/pix/yeast_nw.jpg, 2007.
Infections (primarily bacterial) Drugs/Hormones epinephrine corticosteroids lithium venoms/poisons/toxins Tissue necrosis acute gout burns trauma infarcts Other autoimmune disorders stress severe physical activity pregnancy smoking acute hemorrhage post-splenectomy myeloproliferative disorders Metabolic ketoacidosis uremia eclampsia thyrotoxicosis Causes of Neutrophilia
Demargination of marginated pool of cells doubling of count Release of BM-storage pools left shift Increased cell production sustained neutrophilia Stress (pseudoneutrophilia) Acute Inflammation Chronic Infection Graphic accessed URL http://www.med-ed.virginia.edu/courses/path/innes/wcd/leukocytosis.cfm, 2010. Pathophysiology
EosinophiliaAbsolute count >0.5 x 109/L Causes: • parasites • Helminths • drug treatments • allergies • infections • neoplasms • CML • autoimmune disorders
Basophilia Absolute count >0.15 x 109/L Causes: • CML • allergies • inflammatory disorders • irradiation • viral infections Graphic accessed URL http://healthsystem.virginia.edu/internet/hematology/HessImages/Mature-basophils-100x-website-arrow.jpg, 2006.
MonocytosisAbsolute count >0.8 x 109/L Most commonly seen in conditions with increased cell damage - • Chronic infection [TB, syphilis, protozoal infections, rickettsial infections] • Recovery from agranulocytosis • Post-splenectomy • Strenuous exercise • Subacute bacterial endocarditis
Definition: less than the normal absolute count; greatly influenced by patient age and race. African and Middle Eastern populations Subclasses include mild, moderate and severe Causes Reactions to Drugs BM ablative therapy Infections HIV/Hepatitis Typhoid/ miliary TB Malaria Immune Disorders SLE Neoplasm BM Failure Megaloblastic Anemia Aplastic Anemia Hypersplenism Idiopathic Neutropenia< 2.5 x 109/L
Neutropenia Pathophysiology Defects inside or outside the Bone Marrow • Decreased proliferation [failure of cells - aplasia] • Decreased maturation [insufficient number of precursors undergoing abnormal maturation] • Decreased survival [increased destruction and/or rapid removal of cells] • Distribution [total body pools are normal, circulating numbers are reduced]
Normally: 60-80% circulating lymphs are T-cells [2:1 CD4/CD8] 10-20% are B-lymphs 5-10% are natural killer or NK cells Causes Infections Viral Infectious mononucleosis Bacterial Pertussis Thyrotoxicosis Recovery from acute infections Neoplasm Leukemias Lymphomas LymphocytosisAbsolute count >5.5 x 109/L
Infectious Mononucleosis • Acute, self-limiting, febrile infection of B-cells • Circulating reactive lymphocytes are primary CD8 T-cells • Typically occurs in those age 10-25 years • Fever • Sore throat • Lymphadenopathy • Lethargy • Positive serology – Heterophile antibodies Graphic accessed URL http://www.md.huji.ac.il/mirror/webpath/HEME013.jpg, 2005.
LymphopeniaAbsolute lymphocyte count <0.6 x 109/L • There are three types of abnormalities: • Decreased production • Increased destruction • Changes in distribution
Decreased production SCID = severe combined immunodeficiency Protein-calorie malnutrition Zinc deficiency Increased destruction HIV infection Radiation therapy Neoplastic chemotherapy SLE Redistribution Glucocorticoid therapy Anesthesia TB Influenza Burns Other Hodgkin’s Myasthenia gravis Lymphopenia
Qualitative WBC Disorders Think Morphology Changes Graphics accessed http://us.mms.com/us/mpire/tools/download/wallpapers/2.jpg, http://www.stephengates.com/Blog/uploaded_images/unsignedUser_662.unsignedChar_1170384615063-779906.png, & http://3.bp.blogspot.com/_6B8tPuW7TwQ/Rtw2S9ud0zI/AAAAAAAACiw/tBI6crsT3nU/s400/mandm.jpg, 2009.
Altered Cell Morphology • Nuclear • Pelger-Huet • Hypersegmentation • Cytoplasmic • Alder-Reilly • Chediak-Higashi • May-Hegglin • Gaucher • Niemann-Pick • Mucopolysacchridoses • Toxic Granulation • Vacuolization • Dohle Bodies • Necrobiosis Think Neutrophilia due to Severe Bacterial Infection Peripheral Blood, Wright’s, 100x.
Pelger Huet– an inherited condition resulting in hyposegmentation of granulocyte nuclei with increased density and coarseness of the chromatin.. Don’t confuse this anomaly with a neutrophilic left shift! May-Hegglin- a rare syndrome characterized by leukopenia, variable thrombocytopenia,GIANT PLATELETS,and gray-blue cytoplasmic inclusions in the neutrophils and monocytes [dohle-like bodies] Definitions
Alder-Reilly - an inherited trait characterized by the presence of abnormally large azurophilic and basophilic granulesresembling neutrophilic toxic granulation. Chediak-Higashi- is a genetic disorder that has an equivalent syndrome in mink, cattle, mice, cats, & killer whales. Affected individuals display partial albinism, are very susceptible to common infectious agents, and have white cells demonstratinggiant cytoplasmic granules. Definitions
Gaucher & Niemann-Pickare characterized by the lack of or defective activity of enzymes. In Gaucher disease, there is a lack ofbeta-glucocerebrosidaseand macrophages become laden with glucocerebrosides. In Niemann-Pick, there is deficient activity of lysosomalhydrolase and sphingomyelinase resulting in the accumulation of cholesterol and sphingomyelin in mononuclear phagocytes. Mucopolysaccharidosesare a group of genetically determineddeficiencies of specific enzymesinvolved in the degradation of mucopolysaccharides.Examples: Hurlers Hunter Sanfilippo Definitions
Pelger-Huet & Hypersegmentation Graphics accessed http://evolvels.elsevier.com/section/default.asp?id=1138_ccalvo7_0001, 2008.
May Hegglin Graphic accessed http://evolvels.elsevier.com/section/default.asp?id=1138_ccalvo7_0001, 2008.
Graphic accessed http://evolvels.elsevier.com/section/default.asp?id=1138_ccalvo7_0001, 2008. Alder Reilly
Chediak Higashi Graphic accessed http://evolvels.elsevier.com/section/default.asp?id=1138_ccalvo7_0001, 2008.
Mucopolysacharidoses Graphic accessed ttp://www.academic.marist.edu/~jzmz/topics/bloodsmears/bloodsmears27.html, 2005.
Toxic Granulation & Vacuolization Graphics accessed http://evolvels.elsevier.com/section/default.asp?id=1138_ccalvo7_0001, http://www.mclno.org/webresources/kbase/cellatlas/images/Vacuolated%20Segmented%20Neutrophil.jpg,& http://path.upmc.edu/cases/case53/images/micro2.jpg , 2008.
Graphics accessed http://evolvels.elsevier.com/section/default.asp?id=1138_ccalvo7_0001 & http://www.med-ed.virginia.edu/courses/path/innes/images/wcdjpeg/wcd%20dohle%20x100.jpeg, 2008. Dohle Bodies and Necrobiosis Single or multiple blue cytoplasmic inclusions. They represent remnants of rough endoplasmic reticulum from earlier maturational stages. They are associated with myeloid "left shifts" and are seen in conjunction with toxic granulation. Necrobiotic WBC displays nuclear degradation or karyorrhexis. Indicates cell death in chemotherapy or a poorly preserved specimen. (From Carr JH, Rodak BF: Clinical Hematology Atlas, 2nd ed. Philadelphia: Saunders, 2004.)
Niemann Pick Graphic accessed http://www.nlm.nih.gov/medlineplus/spanish/ency/images/ency/fullsize/1224.jpg, 2001.
Gaucher Graphics accessed http://www.molmed.lu.se/images/gaucher-cell.jpg & http://arttoheartweb.com/images/Van_Gogh_Starry_Night.jpg, 2001.
Lymphocytosis Peripheral Blood, Wright’s, 100x. Bordatella pertussis • Whooping Cough • BUTT CELL Graphic accessedhttp://pathmicro.med.sc.edu/ghaffar/pertussis-lympho.jpg, 1998.
Lymphocytosis • Epstein-Barr Virus • Infectious mononucleosis • Reactive/atypical/variant lymphocytes Graphic accessed http://www.wadsworth.org/chemheme/heme/microscope/imono.htm, 1998.
Check PointHematography Case Studies • Case 1 • Case 10 • Case 14 • Case 25
References • Rodak BF, Fritsma GA, and Doig K. (2007). Hematology Clinical Principles and Applications. St. Louis, Missouri. Saunders Elsevier. Chapter 28 • Anderson SC and Poulsen KB. (2003). Atlas of Hematology. Philadelphia, Pennsylvania. Lippincott Williams Wilkins. • University of Virginia Pathology Hematology • Benign Disorders http://www.med-ed.virginia.edu/courses/path/innes/wcd/benign.cfm Qualitative Disorders http://www.med-ed.virginia.edu/courses/path/innes/wcd/qualitative.cfm