Download
1 / 43
481 likes | 846 Views
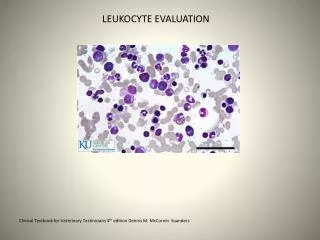
NONMALIGNANT LEUKOCYTE DISORDERS. NONMALIGNANT LEUKOCYTE DISORDERS. Changes in leukocyte concentration and morphology often reflect disease processes and toxic challenge. The type of cell affected depends upon its primary function:

E N D
NONMALIGNANT LEUKOCYTE DISORDERS • Changes in leukocyte concentration and morphology often reflect disease processes and toxic challenge. • The type of cell affected depends upon its primary function: • In bacterial infections, neutrophils are most commonly affected • In viral infections, lymphocytes are most commonly affected • In parasitic infections, eosinophils are most commonly affected.
NONMALIGNANT LEUKOCYTE DISORDERS • Neutrophil disorders • The peripheral neutrophil concentration depends upon • Bone marrow production and release • The rate of neutrophil movement into the tissues • The proportion of circulating to marginating neutrophils • Most benign quantitative abnormalities occur in response to physiologic or pathologic processes • Neutrophilia – an increase in neutrophils • Immediate – may occur without tissue damage or other pathologic stimulus. • Results from a simple redistribution of cells from the marginal pool to the circulating pool
NONMALIGNANT LEUKOCYTE DISORDERS • May occur after violent exercise, epinephrine administration, anesthesia, or anxiety • Is also called shift neutrophilia • Acute neutrophilia – this occurs 4-5 hours after a pathologic stimulus • Results from an increased flow of cells from the bone marrow to the peripheral blood • Bands and metamyelocytes may be seen • Chronic neutrophilia – this follows acute neutrophilia • The bone marrow starts to throw out younger and younger cells (a shift to the left)
NONMALIGNANT LEUKOCYTE DISORDERS • Conditions that are associated with neutrophilia are: • Bacterial infections (most common cause) • This usually causes an absolute neutrophilia (10-19 x109/L) • In severe infections, the bone marrow stores may be depleted and this can result in neutropenia (typically seen in typhoid fever and brucellosis) • Tissue destruction or drug intoxication (tissue infarctions, burns, neoplasms, uremia, gout)
NONMALIGNANT LEUKOCYTE DISORDERS • Leukemoid reaction – this is an extreme neutrophilia with a WBC count > 30 x 109/L • Many bands, metamyelocytes, and myelocytes are seen • Occasional promyelocytes and myeloblasts may be seen. • This condition resembles a chronic myelocytic leukemia (CML), but can be differentiated from CML based on the fact that in leukemoid reactions: • There is no Philadelphia chromosome • The condition is transient • There is an increased leukocyte alkaline phosphatase score (more on this later) • Leukemoid reactions may be seen in tuberculosis, chronic infections, malignant tumors, etc.
NONMALIGNANT LEUKOCYTE DISORDERS • Leukoerythroblastic reaction – in this condition nucleated RBCs and neutrophilic precursors are both found in the peripheral blood • The WBC count may be increased, normal, or decreased • This is associated with myelopthesis (proliferation of abnormal elements in the bone marrow) • Reactive states • With hemorrhage or hemolysis of RBCs, there is increased production of RBCs in the bone marrow and sometimes the granulocyte production also increases. • Corticosteroid therapy
NONMALIGNANT LEUKOCYTE DISORDERS • Neutropenia – this may result from • Decreased bone marrow production • The bone marrow will show myeloid hypoplasia with a decreased M:E ratio • The bone marrow storage pool, and peripheral and marginating pools are all decreased • Immature cells may be thrown into the peripheral blood and those younger than bands are ineffective at phagocytosis. This can lead to overwhelming infections. • This may be due to stem cell failure, radiotherapy, chemotherapy, or myelopthesis. • Ineffective bone marrow production • The bone marrow will be hyperplastic • Defective production is seen in megaloblastic anemias and myelodysplasic syndromes where the abnormal cells are destroyed before they are released from the bone marrow
NONMALIGNANT LEUKOCYTE DISORDERS • Increased cell loss • Early in an infection there is a transient decrease due to increased movement of cells into the tissues • Could be due to an immune mechanism such as production of anti-leukocyte antibodies or PNH • Hypersplenism • Pseudoneutropenia – alterations may occur in the circulating to marginating pools. This may be seen in: • Viral infections • Bacterial infections with endotoxin production • Hypersensitivity reactions
NONMALIGNANT LEUKOCYTE DISORDERS • Periodic or cyclic – is an inherited autosomal dominant disorder in which every 21-30 days there are several days of neutropenia with accompanying infections. This is followed by asymptomatic periods. • Familial – this is benign, chronic, and mild with rare clinical symptoms • Infantile genetic agranulocytosis – this is a rare, congenital, and often fatal disorder in which there is defective bone marrow production of neutrophils. • False – blood drawn into EDTA in which the cells stick to the side of the tube; disintegration of cells due to age from sitting in a tube for too long; cell clumping
NONMALIGNANT LEUKOCYTE DISORDERS • Morphologic and functional abnormalities of neutrophils • Acquired, morphologic – these are reactive, transient changes accompanying infectious states. They include • Toxic granulation • Dohle bodies • Cytoplasmic vacuoles • May also see ingested microorganisms
MORPHOLOGIC NEUTROPHIL CHANGES Vacuolated cell
MORPHOLOGIC NEUTROPHIL CHANGES Toxic granulation
NONMALIGNANT LEUKOCYTE DISORDERS • Inherited functional and/or morphological abnormalities • Pelger- Huet Anomaly – this is a benign, inherited, autosomal dominant abnormality in which the neutrophil nucleus does not segment beyond the bilobular stage (“Prince-nez cells”). • The cells may sometimes resemble bands, but the chromatin is more condensed (mature). • The cells function normally. • Acquired or pseudo Pelger-Huet Anomaly is seen in myeloproliferative and myelodysplastic states
PSEUDO PELGER-HUET ANOMALY Note nuclear maturity
NONMALIGNANT LEUKOCYTE DISORDERS • Alder-Reilly Anomaly – in this disorder all leukocytes contain large, purplish granules (due to partially degraded protein-carbohydrates) in the cytoplasm, but the cells function normally. • This is seen in Hurler’s and Hunter’s syndromes in which there is an incomplete breakdown of mucopolysaccharides
HURLER’S SYNDROME Note the granules
NONMALIGNANT LEUKOCYTE DISORDERS • Chediak-Higashi Anomaly – • This is a rare autosomal recessive disorder in which abnormal lysosomes are formed by the fusion of primary granules. These are seen as grayish-green inclusions • The cells are ineffective in killing microorganisms and affected individuals often die early in life from pyogenic infections.
CHEDIAK-HIGASHI ANOMALY Note abnormal lysosomes
NONMALIGNANT LEUKOCYTE DISORDERS • May-Hegglin Anomaly • This is a rare, autosomal dominant disorder in which the leukocytes contain large basophilic inclusions containing RNA that look similar to Dohle bodies. • It can be differentiated from an infection because toxic granulation is not seen. • The patients also have giant platlets that have a shortened survival time. Because of this, patients may have bleeding problems, but they usually have no other clinical symptoms
MAY-HEGGLIN ANOMALY Basophilic inclusions
NONMALIGNANT LEUKOCYTE DISORDERS • Chronic granulomatous disease • This is a lethal, sex-linked disorder affecting the function of the neutrophil • The neutrophil can function in phagocytosis, but it cannot kill microorganisms because the cells have a defect in the respiratory burst oxidase system. • Affected individuals have chronic infections with organisms that do not normally cause infections in normal individuals • Myeloperoxidase deficiency • This is a benign, autosomal recessive disorder characterized by a lack of myeloperoxidase in the neutrophils
NONMALIGNANT LEUKOCYTE DISORDERS • Affected individuals may have occasional problems with Candida infections, but usually they have no problems with infections because they have other mechanisms to kill microorganisms • Leukocyte adhesion deficiency • This is a rare, autosomal recessive disorder characterized by the absence of leukocyte cell surface adhesion proteins • Because of the lack of the adhesion molecules, the leukocytes have functional defects in: • Chemotaxis • Phagocytosis • Respiratory burst activation • Degranulation • Affected individuals have frequent bacterial and fungal infections and mortality in childhood is high.
NONMALIGNANT LEUKOCYTE DISORDERS • Eosinophil disorders • Eosinophilia may be found in • Parasitic infections • Allergic conditions and hypersensitivity reactions • Eosinophils have low affinity IgE Fc receptors and may be important in modulating immediate hypersensitivity reactions • Cancer • Chronic inflammatory states
NONMALIGNANT LEUKOCYTE DISORDERS • Basophil disorders • Basophilia • Is associated with chronic myeloproliferative disorders (discussed later) • Inflammatory bowel disease • Radiation exposure • Monocyte quantitative and qualitative disorders • Associated with malignancies
NONMALIGNANT LEUKOCYTE DISORDERS • Inherited abnormalities of neutrophils are also seen in monocytes because they originate from a common stem cell: • Chronic granulomatous disease (defective respiratory burst) • Chediak Higashi (abnormal lysosomes caused by fusion of primary granules) • Alder Reilly Anomaly (large purple-blue granules)
NONMALIGNANT LEUKOCYTE DISORDERS • Macrophage disorders • Lipid storage diseases – the cells are unable to completely digest phagocytosed material • Gaucher’s disease – is a recessive autosomal disorder with a deficiency of glucocerebroside • There is an accumulation of lipid in macrophages in lymphoid tissue • This leads to liver and spleen enlargement and destructive bone marrow lesions • Death occurs early in life
NONMALIGNANT LEUKOCYTE DISORDERS • Niemann-Pick Disease – This is an autosomal recessive disorder with a defect in sphingomyelinase • It is often fatal by the age of 3 • Tay Sachs and Sandhoffs diseases – these are autosomal recessive disorders with deficiencies in - hexosaminidase and and - hexosaminidase, respectively • Gangliosides and other glycolipids and mucopolysaccharides accumulate in tissues, especially in the CNS. • This is usually fatal by the age of 4 • Fabry’s, Wolman’s, and Tangier are examples of other lipid storage diseases
NONMALIGNANT LEUKOCYTE DISORDERS • Lymphocyte disorders • Acquired, quantitative • Is usually a self-limited reactive process to infection or inflammation • Both B and T cells are affected • Function is normal, though the morphological process may be heterogenous • With intense proliferation, may have lymphadenopathy or splenomegaly
NONMALIGNANT LEUKOCYTE DISORDERS • Lymphocytosis – may be relative (secondary to neutropenia) or absolute (usually seen in viral infections); if absolute it may or may not be accompanied by a leukocytosis • Infectious mononucleosis (IM) – • This is caused by Epstein-Barr virus infecting B lymphocytes. • The infected B cells may eventually be killed by cytotoxic T cells, though some will continue to harbor the virus in a latent infection. • The reactive lymphocytes seen in the peripheral smear are cytotoxic T cells • The lymphocytosis is accompanied by a leukocytosis
NONMALIGNANT LEUKOCYTE DISORDERS • Cytomegalovirus infection • Leukocytosis with absolute lymphocytosis • Infectious lymphocytosis • Unknown etiology • Leukocytosis with absolute lymphocytosis • 60-97% normal appearing lymphocytes • The increased lymphocytes are mainly T lymphs • Bordetella pertussis infection • Leukocytosis with an absolute lymphocytosis • Due to a redistribution of T lymphocytes from the tissues to the circulation • Lymphocytes are small, normal appearing lymphocytes
NONMALIGNANT LEUKOCYTE DISORDERS • Lymphocytic leukemoid reaction – • Peripheral smear shows increased lymphocytes with younger lymphocytes being seen • Can occur with tuberculosis, chickenpox and the viral diseases discussed above • Plasmocytosis • Plasma cells are rarely seen in the peripheral blood, but they may be found under conditions of intense immune stimulation • Lymphocytopenia – caused by stress, drugs, irradiation, and some diseases
NONMALIGNANT LEUKOCYTE DISORDERS • Congenital qualitative or quantitative disorders – may affect both T and B cells or only one cell type. Most will severely compromise the immune system • Severe combined immunodeficiency system (SCIDS) • This is a heterogenous group of disorders in which both B and T cells are profoundly deficient • In some cases there is no rearrangement of the B cell and T cell receptor genes to produce immunocompetent cells • A bone marrow transplant or gene therapy are the only effective treatments
NONMALIGNANT LEUKOCYTE DISORDERS • Wiskott-Aldrich Syndrome • Is a sex-linked progressive disorder characterized by • Eczema • Thrombocytopenia • Immunodeficiency due to progressive decrease in T cell immunity • There is also an intrinsic B lymphocyte abnormality resulting in an inability to respond to polysaccharide antigens • Most children die before the age of 10 from bleeding and infections • Treatment is a bone marrow transplant
NONMALIGNANT LEUKOCYTE DISORDERS • DiGeorge syndrome • This is characterized by absence or aplasia of the thymus and parathyroid gland • This results in decreased T lymphocytes and death in the first year without thymic grafts • X linked agammaglobulinemia • This is characterized by a block in B lymphocyte maturation leading to a decrease in B lymphocytes and no plasma cells • There is decreased IgM, IgA, and IgG • Treatment is monthly injections with gammaglobulin to prevent infections • Ataxia telangiactasia • This is a cell mediated immune defect with thymic hypoplasia or dysplasia and depletion of T cells
NONMALIGNANT LEUKOCYTE DISORDERS • Acquired immune deficiency syndrome (AIDS) • Caused by human immunodeficiency virus (HIV) • Viral infection results in a selective depletion of T helper cells resulting in opportunistic infections