Download
1 / 25
300 likes | 720 Views
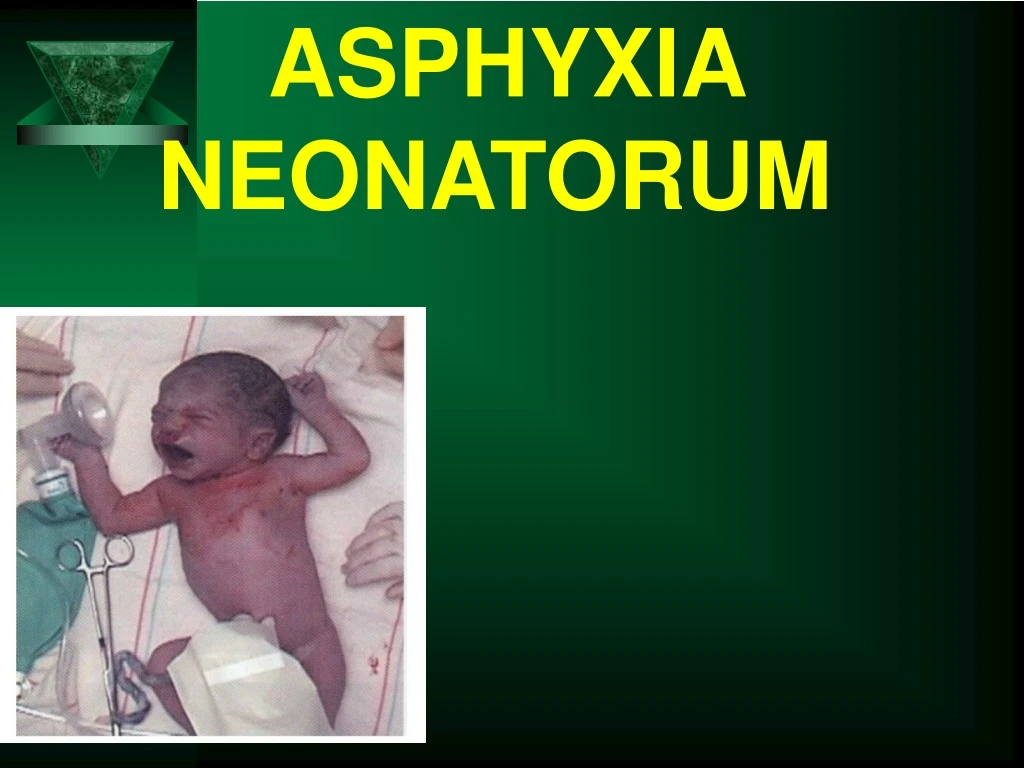
ASPHYXIA NEONATORUM. DEFINITION. Asphyxia neonatorum means non-establishment of satisfactory pulmonary respiration at birth. Its literal meaning is absence of pulse Clinically it is defined as failure to initiate and maintain spontaneous respiration within one minute of birth.

E N D
DEFINITION • Asphyxia neonatorum means non-establishment of satisfactory pulmonary respiration at birth. • Its literal meaning is absence of pulse • Clinically it is defined as failure to initiate and maintain spontaneous respiration within one minute of birth
INITIATION AND MAINTENANCE OF RESPIRATION Change in temperature Proprioceptive stimuli Clamping of the cord Raised PCO2 Lowered PO2 Chemoreceptors Respiratory centre Motor discharge as inspiratoory muscles Initiation of respiration Onset of grasp /cry /sigh Stretching of thoracic cage Re-routing of circulation Normal gaseous exchange
ETIOLOGY • CONTINUATION OF INTRAUTERINE HYPOXIA • BIRTH TRAUMA TO THE NEONATE • PRENATAL AND INTRANATAL MEDICATION TO THE MOTHER
CONTINUATION OF INTRAUTERINE HYPOXIA….Contd • FAILURE IN THE PLACENTAL FUNCTION • Problem in the anatomical separation • Extensive infarcts • Retroplacental haemorrhage • Thin small placenta • Circumvallate placenta • Hypertensive disorders of pregnancy • Supine hypotensive syndrome • Cord compression • True knot in cord • Vascular anomalies in cord
CONTINUATION OF INTRAUTERINE HYPOXIA • MATERNAL HYPOXIC STATES • Anaemia • Eclampsia • Cynotic cardiovascular disorders • Status asthmaticus • Emphysema • Shock • Hypotension
BIRTH TRAUMA MALPRESENTATION • Oblique lie • Breech • Occipito posterior position PROLONGED HEAD COMPRESSION • Malapplied forceps • Ventouse extraction • Prolonged 2nd stage • -Contracted pelvis
BIRTH TRAUMA • Increased intracranial tension • Cerebral edema and congestion • Increased intracranial pressure • Asphyxia.
MEDICATIONS • Prenatal • Intranatal Eg.Morphine ,Pethedine,Anaesthetic agents
CLINICAL FEATURES It depend upon: • Etiology • Intensity and duration of oxygen lack • Plasma Co2 excess • Subsequent acidosis
ACCORDING TO INTENSITY AND DURATION OF OXYGEN LACK CLINICAL FEATURES • Asphyxia Livida (Stage of cyanosis) • Asphyxia pallida (stage of shock)
APGAR SCORING • Total score – 10 , No depression – 7-10 , Moderate depression – 4-6 • Severe depression – 0-3
CLINICAL SEQUENCES OF BIRTH ASPHXIA • Initial response is hyperpnea and hypertension • Primary apnoea • Gasping attempt to breathe • (if unresolved) – secondary apnoea • Bradycardia and shock • Diminished cerebral blood flow • Cerebral haemorrhage • Hypoxic ischaemic encephalopathy • (if severe) – either death or handicap ( if the baby survives)
MANAGEMENT • PROPHYLACTIC • DEFINITIVE
PROPHYLACTIC • Antenatal detection of high risk patients • Scrupulous fetal monitoring, particularly in high risk pregnancy • Intrapartum use of electronic fetal monitoring • Judicious administration of anaesthetic agents and depressant drugs during labor.
Definitive Apgar rating
BABIES WITH APGAR SCORE 7-10 (PINK, BREATHING REGULAR HR > 100). • The oropharynx and the nasopharynx are to be cleared off any mucus by suction • O2 administration • Re-assess the conditions at 5mts
BABIES WITH APGAR SCORE 4-6 [PERIPHERAL CYNOSIS, BREATHING IRREGULAR HR≥100…..Contd • Place under a radiant heater and dry the baby • Baby is put flat or slight head down position • Immediate suction • O2 administration (by bag and mask)
Stimulus to back and sole (gentle rubbing) • If the above measures fail oral suctioning followed by tracheal intubation • The tracheal tube is connected to resuscitation bag through which O2 is administered at the rate of 6-8 litres/ mt • IPPV is maintained at the rate of 30-40 per mt. • Gentle external cardiac massage is performed if HR is < 60/mt
If any history of administration of a central depressant drug to the mother give suitable antidote. Eg. Nalaxone hydrochloride 60g/kg IM (single dose) or 10g/kg i/v – it may have to be repeated. • To combat metabolic acidosis – 8.4% sodiumbicarbonate 1mEq/kg in 5% dextrose (diluted 1:1) is given through umbilical or peripheral vein (at the rate of 1ml/mt)
BABIES WITH APGAR SCORE BELOW 4 (CENTRAL CYANOSIS) • No breathing HR <100] • Tracheal intubation and IPPV must be started immediately • If IPPV is not available gentle mouth to mouth respiration • If mother is received pethedine or morphine within 3hrs of delivery give Nalaxone 10g /kg i/v it may be repeated every 2-3mts.
Complications • Immediate • Delayed • IMMEDIATE • Cardiovascular – HTN, cardiac failure • Renal – acute cortical necrosis, renal failure • Liver function – compromised • GI – Ulcers and necrotising enterocolitis • Lungs – Persistent pulmonary HTN • Brain – Cerebral edema, seizures.
DELAYED • Retarded mental and physical growth • Epilepsy – up to 30% in severe asphyxia • Minimal brain dysfunction • Prognosis • a. It is dependent on normal maturity of the baby • b. Duration and intensity of hypoxia • c. Detection and treatment of fetal distress • d. Facilities for immediate and competent management • c. Detection and treatment of rare congenital anomalies.