Download
1 / 29
290 likes | 305 Views
Get the latest information on the current status of the mumps outbreak in Northwest Arkansas. Learn about the effectiveness of vaccines in preventing mumps and the recommended vaccination schedule. Stay informed and protect yourself and your community.

E N D
Update on Mumps and Current Status of Outbreak in NW Arkansas Cat Waters, BSN Outbreak Response Section Chief Arkansas Department of Health
Vaccines have been proven to prevent millions of illnesses and thousands of deaths each year in the United States Vaccine infographic created by Leon Farrant >5,000,000 31,036
Mumps • Major cause of outbreaks in pre-vaccine era • Vaccination has reduced mumps by 99% in the US • Recently, a few outbreaks have centered around colleges and schools • Particularly in dormitory settings and dense housing • Also in the National Hockey League
Mumps Virus • Paramyxovirus • Enveloped RNA virus • One antigenic type • Rapidly inactivated by UV light, heat, and various chemical agents
Mumps Laboratory Diagnosis • Isolation of mumps virus • Detection of RNA via PCR • Serologic testing • positive IgM antibody • significant increase in IgG antibody between acute and convalescent specimens
Mumps Pathogenesis • Respiratory transmission of virus • (droplet nuclei) • Subclinical infections may transmit • Replication in nasopharynx and regional lymph nodes • Viremia 12-25 days after exposure with spread to tissues • Infective dose – medium. Typical 2o attack rate of 31%
Mumps Clinical Features • Incubation period 14-18 days • Nonspecific prodrome of low-grade fever, headache, malaise, myalgias • Parotitis in 30%-40% • Up to 20% of infections asymptomatic • May present as lower respiratory illness, particularly in preschool-aged children
Mumps Epidemiology • Reservoir Human • Temporal pattern Peak in late winter and spring • Communicability Three days before to four days after onset of active disease
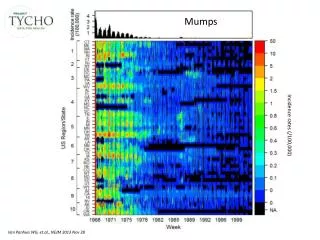
Mumps – United States, 1968- 2005* *2005 provisional data
Mumps - United States, 1980-2003 Age Distribution of Reported Cases
Mumps Immunity • Born before 1957 • Documentation of physician- diagnosed mumps • Serologic evidence of mumps immunity • Documentation of adequate vaccination
Common Symptoms • Parotitis: Inflammation of the salivary glands under the ear • Fever • Headache • Muscle Aches • Fatigue • Loss of Appetite CDC
Classic Swelling of Cheek and Neck (Parotitis) Seen with Mumps CDC Public Health Image Library
Rare but Serious Complications • Inflammation of the: • Testicles • Pancreas • Ovaries • Breast • Encephalitis or Meningitis • Deafness • Male infertility CDC
15% of clinical cases 20%-50% in post- pubertal males 2%-5% 1/20,000 1-3/10,000 CNS involvement Orchitis Pancreatitis Deafness Death Mumps Complications
Epidemiological Characteristics • Persistence in Environment: • Readily inactivated by UV light, formalin, heat, acid • High risk groups: • Post pubertal males – orchitis, atrophy, cancer? • Persons with diabetes • Epidemic Potential: • High – epidemic parotitis • Challenges • Imported cases • immunity may not be lifelong
Mumps Vaccine • Effectiveness 88% after two doses • Duration ofImmunity Generally lifelong • Schedule 1st dose at 12-15 months, 2nd after age 4 and for adults at higher risk • Administered with measles and rubella (MMR) • Developed from the Jeryl Lynn strain (genotype B)
Vaccine Side Effects • Brief achy joints (up to 25% of women) • Uncommon in children • Uncommon symptoms (less than 1%) • Fever • Rash • Itching • Extremely rare events (less than 1/100,000) • Brief orchitis • Mild parotitis • Encephalitis (~1 in 800,000 doses)
Current Status of Outbreak N=769 as of 10/26 N=1,270 as of 11/15 * Numbers for most recent week are provisional
Vaccination Status Among Those Who Have Been Investigated There are 81 more cases under investigation whose vaccine status is not known
Benefits of 2nd (or 3rd) MMR shot • 9 fold lower risk of illness • Milder disease if you do get mumps • Much less likely to transmit to others
What is ADH Doing? • Using the best evidence to control the outbreak • Interviewing all suspect cases and contacts • Excluding under-vaccinated kids from school • Performing vaccination clinics (65 complete, 4 others scheduled) • 4,622 vaccines provided to date • Providing advice to doctors and schools • Communicating to many audiences
Questions / Comments • Appreciation to those that have been involved in the outbreak response!
Cost-Benefit Analysis of Commonly Used Vaccines (Saving per $ invested) Medical Societal* Dollars Dollars VaccineSavedSaved • DTaP 8.50 24.00 • MMR 10.30 13.50 • Hib 1.40 2.00 • Polio vaccine 3.03 6.10 • Varicella 0.90 5.40 • Hepatitis B 2.30 19.80 *Includes work loss, disability and death • Source: CDC, ASTHO
Adult Immunization Recommendations from ACIP • Generally recommended for all adults • Influenza (every year) • Tdap (once as adult then Td booster every ten years • Chickenpox (AKA varicella) • Need physician diagnosed illness, immunity, or 2 doses • HPV (up to 26 years old, 3 doses) • Shingles (AKA zoster) (once ≥ 60 years old) • MMR (up to 59 years old) • Immunity or 2 doses after 1967, unless born prior to 1957 • Pneumococcal vaccine (two different vaccines ≥ 65 years old) • Recommended for certain subgroups (see CDC website for detail) • Hepatitis A (2 doses) • Hepatitis B (3 doses) • Pneumococcal vaccine (below age 65) • Meningococcal vaccine (2 doses)