Download
1 / 38
550 likes | 1.64k Views
INFLAMMATION. CONTENTS. Acute inflammation Chronic inflammation Laboratory test abnormalities in acute and chronic inflammation. ACUTE INFLAMMATION. What are the most common cause of rubor [redness] in Acute inflammation

E N D
CONTENTS • Acute inflammation • Chronic inflammation • Laboratory test abnormalities in acute and chronic inflammation
What are the most common cause of rubor [redness] in Acute inflammation • Arteriolar vasodilatation, due to histamine release from tissue mast cells • What are the most common cause of tumor [swelling] in Acute inflammation • Increased venular permeability primarily due to histamine • What are the most common cause of calor [heat] in Acute inflammation • Arteriolar vasodilatation with increased blood flow due to histamine • What are the most common cause of dolor [pain] in Acute Inflammation • Bradykinin, Prostaglandin G2
What are the most common cause of functio laesa [loss of function] in Acute inflammation • Swelling, Pain • What are the most common histamine-mediated vascular events in Acute inflammation • Arteriolar vasodilatation — > endothelial cell contraction in venules [Basement membrane exposed] — » increased vessel permeability • What are the most common cause of the stroke line, flare, and wheal in the Lewis triple response [dull object is drawn across the skin surface] • Stroke line: histamine-mediated capillary dilatation; Flare at the periphery, neurogenic-induced arteriolar dilatation; Wheal of the stroke line: histamine-mediated increase in vessel permeability
What are the most common sequential neutrophil events in Acute inflammation • Margination [neutrophils pushed to the side in small vessels] -» neutrophil adhesion to venular endothelium [due to adhesion molecule synthesis by neutrophils and endothelial cells] — > emigration out of venules [neutrophil collagenases dissolve type IV collagen in exposed Basement membrane] — » directed chemotaxis [neutrophils have G protein receptors, Gap, causing them to move to the area of infection] — > opsonization of bacteria [bacteria coated by Immunoglobulin G and C3b] — > phagocytosis of opsonized bacteria [internalization of bacteria] — > killing of bacteria
What are the most common chemical mediators responsible for neutrophil synthesis of adhesion molecules [GDI I/ GDI 8 complex with glycoproteins and PrPz integrins] and endothelial cell leukocyte and intercellular adhesion molecules • Complement component 5a and Leukotriene B4 (neutrophils only), Interleukin-1 and Tumor necrosis factor(neutrophils and endothelial cell synthesis of adhesion molecules) [Endothelial cell leukocyte adhesion molecule-1 synthesized in endothelial cells binds to neutrophil receptors. Intercellular adhesion molecule-1 adheres to neutrophil and lymphocyte receptors.] • What are the most common clinical findings in J2 integrin deficiency • Failure of separation of the umbilical cord in the newborn and absence of acute inflammatory cells in the umbilical cord • What are the most common chemical mediators serving as chemotactic agents • Complement component 5a, Leukotriene B4, Interleukin-8, bacterial products
What are the most common causes of decreased adhesion molecule synthesis • Corticosteroids, Catecholamines, Lithium [This increases the total neutrophil count by releasing the marginating pool.] • What are the most common pathologic cause of increased adhesion molecule synthesis • Endotoxemia in gram-negative sepsis [This lowers the total neutrophil count (absolute neutropenia).] • What are the most common cause of the low total white blood cell count in black people • Increased marginating pool of neutrophils, due to increased neutrophil adhesion [Normally, the peripheral circulating pool of neutrophils (pool counted in a complete blood cell count) and marginating pool are about equal.]
What are the most common type of interstitial fluid accumulation in Acute Inflammation • Exudate containing neutrophils, red blood cells, fibrin, and digested debris • What are the most common Oxygen-dependent bactericidal systems in neutrophils and monocytes • Oxygen-dependent Myeloperoxidase system (most potent system), generation of superoxide free radicals [The Myeloperoxidase system requires oxygen, Nicotinamide adenine dinucleotide phosphate, NADPH oxidase (converts O2 to superoxide), NADPH (cofactor), Superoxide dismutase (converts superoxide into peroxide), and chloride ions (Myeloperoxidase catalyzes the reaction between chloride ions and peroxide to form bleach, which kills bacteria.] • What are the most common Oxygen-independent bactericidal systems in neutrophils, monocytes, and macrophages • pH changes in phagolysosomes, lysosomal enzymes
What are the most common source of NADPH in the O2-dependent Myeloperoxidase system • The pentose phosphate shunt [glucose 6-phosphate dehydrogenase is the key enzyme] is the major source of NADPH in the body • What are the most common disease associated with deficiency of NADPH oxidase • Chronic granulomatous disease (CGD) of childhood [It is a Sex-linked recessive disease. Deficiency of the enzyme leads to absence of peroxide and inability to form bleach, even though chloride ions and Myeloperoxidase are present in the phagolysosome.] • What are the most common screening test for Chronic granulomatous disease • Nitroblue tetrazolium (NET) test [Normally, conversion of molecular O2 into superoxide free radicals emits energy (called the respiratory burst). When colorless nitroblue tetrazolium is added to a test tube containing neutrophils, it is phagocytosed and superoxide converts nitroblue tetrazolium into a colored dye. In Chronic granulomatous disease the respiratory burst is absent.]
What are the most common cause of death in Chronic Granulamatous Disease • Sepsis due to catalase-positive bacteria (e.g., Staphylococcus aureus) [Catalase from the bacteria destroys the peroxide generated by the organism, hence neutrophils are deprived of peroxide to synthesize bleach necessary to kill the bacteria.] • What are the most common genetic disease associated with a defect in microtubule polymerization • Chediak-Higashi syndrome [It is an Autosomal recessive disease. Inability to polymerize microtubules impairs leukocyte motility (defective chemotaxis) and also results in delayed fusion of lysosomes with phagosomes to form phagolysosomes (responsible for the giant lysosomes noted in the peripheral blood leukocytes).] • What are the most common cells involved in Acute inflammation associated with bacteria, viruses, and allergic reactions • Neutrophils, lymphocytes, and eosinophils, respectively
What are the most common vasoactive amines • Histamine and Serotonin [Histamine is preformed in the granules of mast cells and basophils. Serotonin is present in the dense bodies of platelets. Both are vasodilators and increase vessel permeability.] • What are the most common plasma-derived proteases • Coagulation factors, Kinins [These proteases (and complement) have a cascade type of system, in which one activated product activates the next product.] • What are the most common complement factors involved in Acute inflammation • C3a, Complement component 3a [anaphylatoxin; direct stimulation of mast cell release of histamine], C3b [opsonization], C5a [adhesion molecule synthesis, chemotactic agent, anaphylatoxin]
What are the most common plasma-derived protease that activates the intrinsic clotting system, kinin system [source of bradykinin], and the fibrinolytic system [source of plasmin] • Hageman factor XII • What are the most common drug that blocks the synthesis of both prostaglandins and leukotrienes • Corticosteroids [They block phospholipase, which prevents cell membrane release of arachidonic acid. In Acute inflammation, prostaglandins are vasodilators and increase vessel permeability. Leukotriene B4 enhances adhesion molecule synthesis in neutrophils and is a chemotactic agent. Leukotriene C4,-D4,-E4 are potent vaso- and bron-choconstrictors and increase vessel permeability.] • What are the most common drugs that block cyclooxygenase and the formation of prostaglandins • Aspirin and Nonsteroidal anti-inflammatory drugs (NSAIDs)
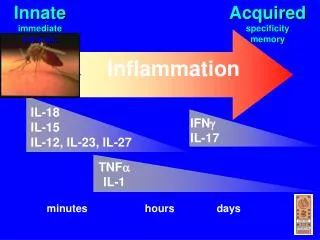
What are the most common sources of Interleukin-1 and Tumor necrosis factor • Macrophages and Endothelial cells • What are the most common site for synthesis of acute phase reactants • Liver [Interleukin-1 and Tumor necrosis factor stimulate hepatocytes to synthesize various proteins (fibrinogen, C-reactive protein, complement, coagulation factors) and reduce synthesis of transferrin and albumin.] • What are the most common stimulus for fever in Acute inflammation • Interleukin-1 and Tumor necrosis factor [They stimulate the synthesis of prostaglandin in the hypothalamus, which in turn activates the thermoregulatory center.]
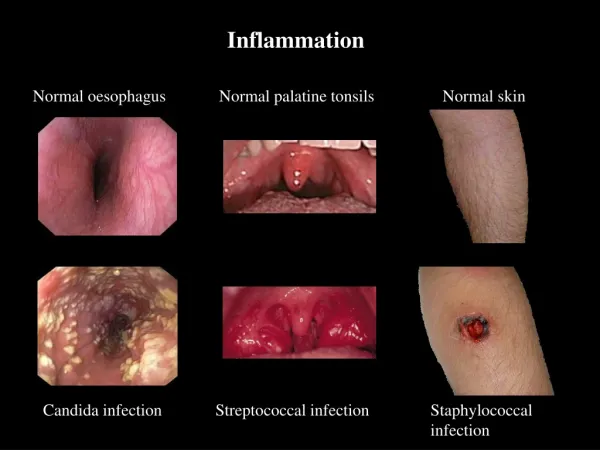
What are the most common benefits of fever • It right-shifts the Oxygen dissociation curve (releases more Oxygen to tissue) and hinders viral and bacterial reproduction • What are the most common expression of serous inflammation [thin, watery exudate] • Blister fluid (second-degree burn) • What are the most common expression of catarrhal (phlegmonous) inflammation [excessive mucous secretions] • Runny nose in the common cold
What are the most common expression of flbrinous inflammation [exudate rich in fibrin, producing a "bread and butter" appearance of a serosal surface] • Fibrinous pericarditis (rheumatic fever, uremia, Systemic Lupus Erythematsous) • What are the most common expression of suppurative inflammation [collection of pus in a localized area] • Abscess (most commonly Staphylococcus aureus) [Abscesses are most commonly located on the skin.] • What are the most common expression of cellulitis [thin exudate that spreads in subcutaneous tissue] • Cellulitis due to Streptococcus pyogenes
What are the most common disorder associated with pseudo-membranous inflammation [toxin-induced membrane along a mucosal surface] • Pseudomembranous colitis due to Clostridium difficile [Pseudomembranes also occur in diphtheria.] • What are the most common outcome of Acute inflammation • Organization and repair with scar tissue formation [Resolution (restoration back to normal without scar formation) and Chronic inflammation are less frequent outcomes].
What are the most common sequential reactions in healing by primary intention [wound edges are apposed] • Wound fills with blood clot — > neutrophils emigrate into wound (24 hours) — > squamous cells migrate below clot and form a continuous lining (1-2 days) — » macrophages replace neutrophils in wound; granulation tissue begins forming (vascular tissue with fibroblasts; 3 days) — » granulation tissue peaks (5 days) — » tensile strength of wound from type III collagen 10% (7-10 days) — » maximal tensile strength of 80% (3 months; type III collagen replaced by type I collagen) • What are the most common differences between secondary and primary intention wounds • Secondary intention wounds are not apposed and myofibroblasts bring the wound edges together [Myofibroblasts have contractile properties.]
What are the most common cell types involved in wound repair • Macrophages (growth factors, phagocytosis of debris), Fibroblasts (collagen synthesis in granulation tissue), Endothelial cells (vessels in granulation tissue) • What are the most common chemical mediators involved in wound repair • Fibronectin (chemotactic for above cell types; molecular glue; promotes angiogenesis) and basic fibroblast growth factor (major promoter of angiogenesis)
What are the most common cause of poor wound repair • Infection [Other causes: malnutrition, scurvy, zinc deficiency (zinc is a cofactor in collagen-ase in remodeling of collagen), copper deficiency (copper is a cofactor in lysyl oxidase involved in forming cross-links in collagen), corticosteroids (interfere with collagen synthesis), Diabetes Mellitus (glucose is a culture medium for bacteria; ischemia; impaired chemotaxis), Ehlers-Danlos syndrome (defect in collagen), Marfan's syndrome (defect in flbrillin in elastic tissue).] • What are the most common source of collagen in organization and repair of liver tissue • Ito cell [It normally serves as a storage depot for retinoic acid, but in liver injury, it synthesizes collagen.]
What are the most common site injured in the kidney • Renal medulla [Only 10% of the 20-25% of the cardiac output devoted to the kidneys is directed to the medulla (cortex receives 90%), hence it lacks Oxygen for effective repair of tissue.] • What are the most common reserve cell responsible for organization and repair in the lungs • Type II pneumocyte [This cell replaces type I pneumocytes and synthesizes surfactant.] • What are the most common type of tissue involved in cardiac muscle repair • Scar tissue [Cardiac muscle is permanent tissue, hence it is replaced with scar tissue.]
What are the most common type of organization and repair in injury of the Central nervous system • Gliosis [Gliosis is equivalent to scar tissue formation outside the central nervous system. Astrocytes are analogous to fibroblasts. Astrocyte proliferation and extension of their protoplasmic processes provide support to the tissue.] • What are the most common type of organization and repair of peripheral nerves • Wallerian degeneration [Axonal regeneration (axonal sprouts from the proximal end of the nerve) and myelination (from Schwann cells) occur after transection of a nerve.]
QUESTION • Which of the following cells or chemical mediators has the LEAST significant role in the first 24 hours of Acute inflammation? • (A) Neutrophils • (B) Histamine • (C) C5a • (D) Monocytes • (E) Bradykinin
What are the most common cause of Chronic Inflammation • Acute Inflammation • What are the most common types of diseases that are chronic at their inception • Autoimmune disease, Granulomatous inflammation • What are the most common immunoglobulin associated with Chronic Inflammation • Immunoglobulin G [Immunoglobulin M is the most common Immunoglobulin associated with Acute inflammation before isotype switching after a week to 10 days.] • What are the mosr common cell type in CIhronic Inflammation • Monocyte
What are the most common functions of monocyte • Transforms into a macrophage (fixed or wandering), contains growth factors, secretes Interleukin-1 and Tumor necrosis factor, synthesizes complement and nitric oxide (potent vasodilator), kills microbial pathogens (Oxygen-dependent Myeloperoxidase system), processes antigen, key cell in delayed hypersen-sitivity reactions, destroys intracellular microbial pathogens (e.g., Tuberculosis, systemic fungi, Legionella), reservoir cells for Human Immunodeficiency Virus [Other cell types in Chronic inflammation include lymphocytes, fibroblasts, endothelial cells, plasma cells.] • What are the most common cell type in syphilis • Plasma cells surrounding inflamed arterioles (called endarteritis obliterans)
What are the most common cell type responsible for producing epithelioid and multinucleated giant cells in a granuloma • Macrophage [Activated macrophages resemble epithelial cells (epithelioid). Epithelioid cells fuse together to form multinucleated giant cells when they die.] • What are the most common cause of a sinus tract [communication with the skin surface] • Skin abscess due to Staphylococcus aureus • What are the most common cause of fistula in the Gastrointestinal tract [communication between two hollow organs] • Diverticulosis, Crohn's disease • What are the most common type of repair in Chronic Inflammation • Fibrosis (scar tissue formation)
QUESTIONS • Which of the following is more likely to represent chronic rather than Acute Inflammation? • (A) Rheumatoid arthritis • (B) Appendicitis • (C) Streptococcus pneumonias • (D) Pneumonia • (E) Rhinitis in a common cold • (F) Bee sting site
Laboratory Test abnormalities in Acute and Chronic inflammation
What are the most common neutrophil response in Acute Inflammation • Absolute neutrophilic leukocytosis [increased neutrophil count in a Complete Blood Cell count], Left shift [5:10 band neutrophils in a 100 White Blood Cell differential count], Toxic granulation [prominence of azurophilic granules containing Myeloperoxidase in neutrophils], phagolysosomes [evidence of phagocytosis], Dohle bodies [dull gray cytoplasmic inclusions representing dilated endoplasmic reticulum] • What are the most common Complete Blood Cell count finding in viral infections • Absolute lymphocytosis [increased number of lymphocytes in a 100 cell differential count] [Some infections produce normal-appearing lymphocytes (e.g., infectious lymphocytosis), while others produce antigenically stimulated (atypical) lymphocytes (e.g., infectious mononucleosis, viral hepatitis). Some bacterial infections produce a lymphocytosis, particularly those due to Bordetella pertussis.]
What are the most common complete blood cell count finding in Type I hypersensitivity reactions and invasive helminthic infections • Eosinophiha [Protozoal infections do not produce eosinophilia. Pinworm infections do not produce eosinophilia, since they are non-invasive. Strongyloidiasis, hookworm infections, etc., do produce eosinophilia.] • What are the most common complete blood cell count finding in Chronic Inflammation • Monocytosis [Monocytes are the primary cell of Chronic Inflammation]
What ar the most common anemia in Chronic Inflammation • Anemia of chronic inflammation [Iron is delivered to macrophages by neutrophil-derived lactoferrin, where it is blocked from being used for erythropoiesis. This lowers the serum iron. Increased iron stores reduce liver synthesis of transferrin (binding protein for iron); hence the total iron-binding capacity (TIBC) is also decreased.] • What are the most common factors increasing/ decreasing the Erythrocyte sedimentation ratio (ESR) • Fibrinogen and gamma globulins [Both of these produce rouleaux ("stack of coins" effect), which increases the rate of settling of Red Blood Cells in a test tube over a 1-hour period. Inflammation and anemia increase the ESR. In sickle cell anemia and polycythemia, the ESR is zero, since abnormally shaped red blood cells and excess numbers of red blood cells do not settle well.]
What are the most common reason for ordering a Serum Protein Electrophoresis • Rule out a monoclonal gammopathy (e.g., multiple myeloma) [Monoclonal gammopathys are spikes in the -y-globulin region that are due to synthesis of a single Immunoglobulin from a single clone of plasma cells.] • What are the most common peaks identified in a routine Serum Protein Electrophoresis • In sequential order from anode to cathode: Prealbumin, Albumin, a^globulins (contain a,a-antitrypsin), a2-globulins (contain haptoglobin, <xz-macroglobulin), ^-globulins (contain transferrin, complement, Low density lipoprotein), ^-globulins (contain IgG, IgA, IgM, IgD, IgE), and C-reactive protein • What are the most common functions of prealbumin (transthyretin) • Complexes with retinal-binding protein to bind both thyroxine and retinoic acid
What are the most common functions of albumin • Due to a strong negative charge, it avidly binds cations (calcium, magnesium), drugs, fatty acids, and unconjugated bilirubin. It is also responsible for 80% of the oncotic pressure in plasma (keeps fluid in vessels) • What are the most common cause of hypocalcemia • Hypoalbuminemia [Albumin binds 40% of the calcium. Measured total calcium is calcium bound to albumin, calcium bound to phosphate/sulfate (13%), and free, ionized calcium (47%). To correct the total calcium for the degree of hypoalbuminemia, the following formula is useful: Corrected calcium = total calcium - serum albumin + 4.]
What are the most common function of Alpha-1 Antitrypsin • An antiprotease that neutralizes elastase in tissue [Genetic deficiency of Alpha-1 Antitrypsin or inactivation of Alpha-1 Antitrypsin by cigarette smoke allows elastases from neutrophils in the lung to destroy the elastic tissue support of the airways, leading to chronic obstructive pulmonary disease.] • What are the most common serum protein electrophoresis finding in Alpha-1 Antitrypsin deficiency • Flat a,-peak [Alpha 1- Antitrypsin deficiency is an Autosomal recessive disease that may produce liver disease in children or panacinar emphysema in adults that is limited to the lower lobes.] • What are the most common function of haptoglobin • Binds to Hemoglobin to form a Hemoglobin-haptoglobin complex that is phagocytosed by macrophages [This salvages the amino acids and iron that would be lost by eliminating Hemoglobin in the urine. Low haptoglobin levels are an excellent marker of intravascular hemolysis.]
What are the most common location on a Serum protein electrophoresis for Immunoglobulin A • The junction of the p and y peaks [Immunoglobulin A is increased in alcoholic cirrhosis, hence filling in the valley between the two peaks results in a single fj--y peak.] • What are the most common Immunoglobulin responsible for the size of the y-globulin peak • IgG [The concentration of immunoglobulins in descending order are IgG, IgA, IgM, IgD, and IgE. Hence, an increase in IgG automatically increases the size of the -/-globulin peak.]
What are the most common cause of a polyclonal gammopathy • Chronic inflammation with an increase in IgG [IgG is the primary Immunoglobulin of chronic inflammation hence its increase by multiple clones of plasma cells results in a diffuse increase in the size of the -y-elobulin peak.] • What are the most common cause of a flat •/-globulin peak • Decreased concentration of IgG [Hypogammaglobulinemia, which includes low IgG levels, is noted in Bruton's agammaglobulinemia, nephrotic syndrome, chronic lymphocytic leukemia] • What are the most common clinical usefulness of C-reactive protein • Marker of bacterial infection versus viral infection [C-reactive is only increased in bacterial infections and conditions with excessive necrosis (e.g., Acute myocardial infarction.]
QUESTION • Which of the following would more likely be noted in an acute rather than chronic bacterial infection? • (A) Polyclonal gammopathy • (B) Left-shifted smear • (C) Monocytosis • (D) Macrophage blockade of iron • (E) Increased ESR