Download
1 / 4
60 likes | 260 Views
OVERVIEW OF HIV/AIDS & TB IN NAMIBIA. The 9 th Advanced HIV COURSE-AIX-EN-PROVENCE-FRANCE 07 th -9 th september 2011 Dr. Mgori,NK-(MD,FMMED cand ). Population 1.8 million 70% of the world’s estimated 40 million people living with HIV/AIDS are located in Sub-Saharan Africa

E N D
OVERVIEW OF HIV/AIDS & TB IN NAMIBIA • The 9th Advanced HIV COURSE-AIX-EN-PROVENCE-FRANCE • 07th-9thseptember 2011 Dr. Mgori,NK-(MD,FMMED cand)
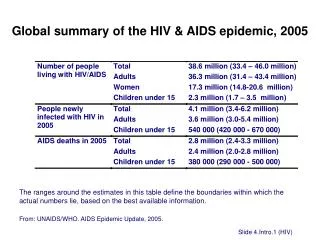
Population 1.8 million 70% of the world’s estimated 40 million people living with HIV/AIDS are located in Sub-Saharan Africa Overall HIV prevalence in Namibia stands at 17.8%. In 2007, Namibia’s estimated tuberculosis (TB) incidence rate of 767 cases per 100,000 population was the fourth highest in Africa, and more than twice the African regional average The TB prevalence of 532 cases per 100,000 population and TB mortality of 102 cases per 100,000 population are also above average for the region About 67 percent of newly registered TB patients are HIV positive SUMMARY
5.Develop and Improvement Theory • If the all nursing staff are educated about the need for providing IPT, then they are likely to provide it • If the screening tools for IPT are provided in all the consulting rooms, then providers (doctors and all nurses) are more likely to screen for IPT • If the screening tools for TB are made available, then the providers are likely to screen for TB and identify those eligible for IPT • If the data clerk provides information on the correct recording of IPT data, then providers are more likely to document IPT when they provide it 1.Getting Started 6.Test the Improvement Theory • Review of routine Quality Management Performance Data by the Provider Team revealed that: • Of the 11 quality indicators routinely monitored by the Quality Program IPT performance score (22%) was the lowest in the last review period (December 2009) • IPT scores were generally very low at all previous quality monitoring review periods • The interventions were tried on patients registering with the ARV clinic over one month from January 15 to February 15 2010 • Data was collected over the intervention period to monitor for number of patients: • Eligible for IPT • Eligible for IPT commenced on IPT during the intervention period • From previous cohort who returned to pick up IPT refills • From previous cohort who failed to come for refills • Stopped by providers due to side effects • Cumulative number of patients on IPT at the clinic AIM Statement To improve the provision of TB Isoniazid Preventive Therapy to eligible patients from a baseline of 22% in December2009 to at least 50% by June 2010 2.Assembling the Team • A QI Project team was established : • Medical Officer. Team lead and chair • Registered Nurse-Project Secretary • Team members: • Sister -In-Charge • Pharmacist • Data Clerk • Community Counselor • Expert Patient 3.Investigate the current Process • July to December 09 performance data were presented at a weekly departmental meeting. • Data for all previous quality indicator performance scores was reviewed • Staff members were asked to comment on the data • It was agreed that “IPT “ be taken up as a QI project • A team was selected to spearhead the project. • 94 patients were newly registered for HIV care for between Jan 15 and Feb 15 2010 • 80 patients were started on IPT in that period • This translated to a performance of 85% • From Feb15 2010 IPT was now offered to all eligible pre-HAART patients by all the nurses • Given the success of the pilot phase, the project was further expanded to include the patients on HAART as from 15 March 2010 Start of QI project • The doctor gave a presentation to all the clinic nurses on screening for IPT eligibility and how to prescribe IPT • A screening tool for TB was made available in all consulting rooms • A screening tool for IPT was availed for all providers • Data clerk gave a presentation on documentation in the patient’s file to improve documentation • Expert patient provided intensified Health Education to patients on IPT and TB in order to clear the thematic myths and misconceptions on IPT identified in the Focus Group Discussions 4.Identify Potential Solutions 9.Establish Future Plans • A red sticker was stuck on passports of patients on IPT for ease of identification and follow up on adherence and monitor completion rates • During H/E patients were shown samples of IPT and CPT for differentiation • Staff were encourage to record on the TB column in the file if IPT had been taken prior (e.g. IPT 2006) • Pharmacist on the QI team will continue updating the team regularly on IPT progress during staff meetings FOR FURTHER INFO CONTACT: hivqualnam@nacop.net www.healthqual.org