Download
1 / 1
10 likes | 112 Views
Follow-up III DE and PSA in 4 months and then yearly. Follow-up II DE and PSA in 6 months and then yearly. Men aged 40-75 years-old with more than 10 years of life expectancy. Follow-up I; schedulled DE+ PSA:

E N D
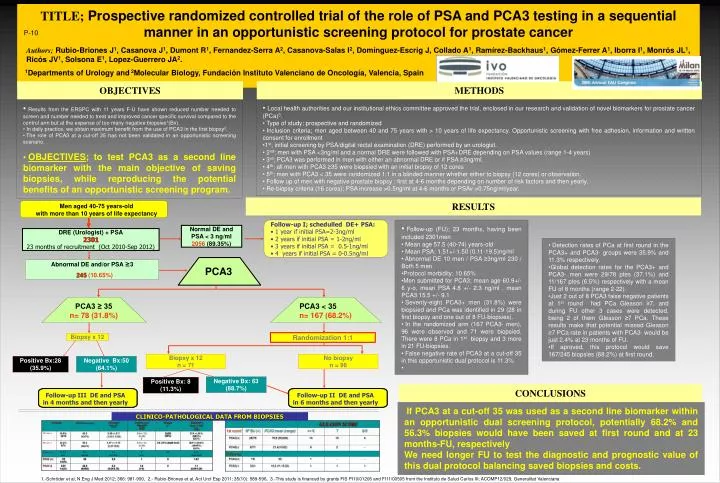
Follow-up III DE and PSA in 4 months and then yearly Follow-up II DE and PSA in 6 months and then yearly Men aged 40-75 years-old with more than 10 years of life expectancy • Follow-up I; schedulled DE+ PSA: • 1 year if initial PSA=2-3ng/ml • 2 years if initial PSA = 1-2ng/ml • 3 years if initial PSA = 0.5-1ng/ml • 4 years if initial PSA = 0-0.5ng/ml Normal DE and PSA < 3 ng/ml 2056 (89.35%) DRE (Urologist) + PSA 2301 23 months of recruitment (Oct 2010-Sep 2012) Abnormal DE and/or PSA ≥3 245(10.65%) PCA3 PCA3 ≥ 35 n= 78 (31.8%) PCA3 < 35 n= 167 (68.2%) Randomization 1:1 Biopsy x 12 Biopsy x 12 n = 71 No biopsy n = 96 Positive Bx:28 (35.9%) Negative Bx:50 (64.1%) Negative Bx: 63 (88.7%) Positive Bx: 8 (11.3%) TITLE;Prospective randomized controlled trial of the role of PSA and PCA3 testing in a sequential manner in an opportunistic screening protocol for prostate cancer P-10 Authors; Rubio-Briones J1, Casanova J1, Dumont R1, Fernandez-Serra A2, Casanova-Salas I2, Domínguez-Escrig J, Collado A1, Ramírez-Backhaus1, Gómez-Ferrer A1, Iborra I1, Monrós JL1, Ricós JV1, Solsona E1, Lopez-Guerrero JA2. 1Departments of Urology and 2Molecular Biology, Fundación Instituto Valenciano de Oncología, Valencia, Spain OBJECTIVES METHODS • Results from the ERSPC with 11 years F-U have shown reduced number needed to screen and number needed to treat and improved cancer specific survival compared to the control arm but at the expense of too many negative biopsies1(Bx). • In daily practice, we obtain maximum benefit from the use of PCA3 in the first biopsy2. • The role of PCA3 at a cut-off 35 has not been validated in an opportunistic screening scenario. • OBJECTIVES; to test PCA3 as a second line biomarker with the main objective of saving biopsies, while reproducing the potential benefits of an opportunistic screening program. • Local health authorities and our institutional ethics committee approved the trial, enclosed in our research and validation of novel biomarkers for prostate cancer (PCa)3. • Type of study; prospective and randomized • Inclusion criteria; men aged between 40 and 75 years with > 10 years of life expectancy. Opportunistic screening with free adhesion, information and written consent for enrollment • 1st; initial screening by PSA/digital rectal examination (DRE) performed by an urologist. • 2nd; men with PSA <3ng/ml and a normal DRE were followed with PSA+DRE depending on PSA values (range 1-4 years) • 3rd; PCA3 was performed in men with either an abnormal DRE or if PSA ≥3ng/ml. • 4th; all men with PCA3 ≥35 were biopsied with an initial biopsy of 12 cores • 5th; men with PCA3 < 35 were randomized 1:1 in a blinded manner whether either to biopsy (12 cores) or observation. • Follow up of men with negative prostate biopsy ; first at 4-6 months depending on number of risk factors and then yearly. • Re-biopsy criteria (16 cores); PSA increase >0.5ng/ml at 4-6 months or PSAv >0.75ng/ml/year. RESULTS • Follow-up (FU); 23 months, having been included 2301men • Mean age 57.5 (40-74) years-old • Mean PSA; 1.51+/-1.50 (0.11-19.5)ng/ml • Abnormal DE 10 men / PSA ≥3ng/ml 230 / Both 5 men • Protocol morbidity; 10.65% • Men submitted for PCA3; mean age 60.9+/- 6 y-o, mean PSA 4.8 +/- 2.3 ng/ml , mean PCA3 15.5 +/- 9.1 • Seventy-eight PCA3+ men (31.8%) were biopsied and PCa was identified in 29 (28 in first biopsy and one out of 8 FU-biopsies). • In the randomized arm (167 PCA3- men), 96 were observed and 71 were biopsied. There were 8 PCa in 1st biopsy and 3 more in 21 FU-biopsies. • False negative rate of PCA3 at a cut-off 35 in this opportunistic dual protocol is 11.3% • Detection rates of PCa at first round in the PCA3+ and PCA3- groups were 35.9% and 11.3% respectively. • Global detection rates for the PCA3+ and PCA3- men were 29/78 ptes (37.1%) and 11/167 ptes (6.5%) respectively with a mean FU of 8 months (range 2-22). • Just 2 out of 8 PCA3 false negative patients at 1st round had PCa Gleason ≥7, and during FU other 3 cases were detected, being 2 of them Gleason ≥7 PCa. These results make that potential missed Gleason ≥7 PCa rate in patients with PCA3- would be just 2.4% at 23 months of FU. • If aproved, this protocol would save 167/245 biopsies (68.2%) at first round, CONCLUSIONS If PCA3 at a cut-off 35 was used as a second line biomarker within an opportunistic dual screening protocol, potentially 68.2% and 56.3% biopsies would have been saved at first round and at 23 months-FU, respectively We need longer FU to test the diagnostic and prognostic value of this dual protocol balancing saved biopsies and costs. CLINICO-PATHOLOGICAL DATA FROM BIOPSIES 1.-Schröder et al, N Eng J Med 2012; 366: 981-990, 2.- Rubio-Briones et al, Act Urol Esp 2011; 35(10): 589-596, 3.-This study is financed by grants FIS PI10/01206 and FI11/00505 from the Instituto de Salud Carlos III; ACOMP12/029, Generalitat Valenciana






















