Download
1 / 1
10 likes | 125 Views
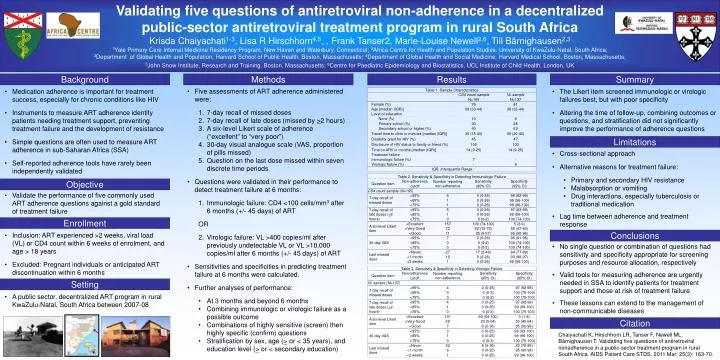
Validating five questions of antiretroviral non-adherence in a decentralized public-sector antiretroviral treatment program in rural South Africa Krisda Chaiyachati 1-3 , Lisa R Hirschhorn 4,5 , , Frank Tanser2, Marie-Louise Newell 2,6 , Till Bärnighausen 2,3

E N D
Validating five questions of antiretroviral non-adherence in a decentralized public-sector antiretroviral treatment program in rural South Africa Krisda Chaiyachati1-3, Lisa R Hirschhorn4,5, , Frank Tanser2, Marie-Louise Newell2,6, Till Bärnighausen2,3 1Yale Primary Care Internal Medicine Residency Program, New Haven and Waterbury, Connecticut; 2Africa Centre for Health and Population Studies, University of KwaZulu-Natal, South Africa; 3Department of Global Health and Population, Harvard School of Public Health, Boston, Massachusetts; 4Department of Global Health and Social Medicine, Harvard Medical School, Boston, Massachusetts; 5John Snow Institute, Research and Training, Boston, Massachusetts; 6Centre for Paediatric Epidemiology and Biostatistics, UCL Institute of Child Health, London, UK Background Methods Results Summary • Five assessments of ART adherence administered were: • 7-day recall of missed doses • 7-day recall of late doses (missed by >2 hours) • A six-level Likert scale of adherence (“excellent” to “very poor”) • 30-day visual analogue scale (VAS, proportion of pills missed) • Question on the last dose missed within seven discrete time periods. • Questions were validated in their performance to detect treatment failure at 6 months: • Immunologic failure: CD4 <100 cells/mm3 after 6 months (+/- 45 days) of ART • OR • Virologic failure: VL >400 copies/ml after previously undetectable VL or VL >10,000 copies/ml after 6 months (+/- 45 days) of ART • Sensitivities and specificities in predicting treatment failure at 6 months were calculated. • Further analyses of performance: • At 3 months and beyond 6 months • Combining immunologic or virologic failure as a possible outcome • Combinations of highly sensitive (screen) then highly specific (confirm) questions • Stratification by sex, age (> or < 35 years), and education level (> or < secondary education) • Medication adherence is important for treatment success, especially for chronic conditions like HIV • Instruments to measure ART adherence identify patients needing treatment support, preventing treatment failure and the development of resistance • Simple questions are often used to measure ART adherence in sub-Saharan Africa (SSA) • Self-reported adherence tools have rarely been independently validated • The Likert item screened immunologic or virologic failures best, but with poor specificity • Altering the time of follow-up, combining outcomes or questions, and stratification did not significantly improve the performance of adherence questions Limitations • Cross-sectional approach • Alternative reasons for treatment failure: • Primary and secondary HIV resistance • Malabsorption or vomiting • Drug interactions, especially tuberculosis or traditional medication • Lag time between adherence and treatment response Objective • Validate the performance of five commonly used ART adherence questions against a gold standard of treatment failure Enrollment • Inclusion: ART experienced >2 weeks, viral load (VL) or CD4 count within 6 weeks of enrolment, and age > 18 years • Excluded: Pregnant individuals or anticipated ART discontinuation within 6 months Conclusions • No single question or combination of questions had sensitivity and specificity appropriate for screening purposes and resource allocation, respectively • Valid tools for measuring adherence are urgently needed in SSA to identify patients for treatment support and those at risk of treatment failure • These lessons can extend to the management of non-communicable diseases Setting • A public sector, decentralized ART program in rural KwaZulu-Natal, South Africa between 2007-08 Citation Chaiyachati K, Hirschhorn LR, Tanser F, Newell ML, Bärnighausen T. Validating five questions of antiretroviral nonadherence in a public-sector treatment program in rural South Africa. AIDS Patient Care STDS. 2011 Mar; 25(3): 163-70.