Download
1 / 39
400 likes | 662 Views
MAKASSED EXPERIENCE IN MANAGEMENT OF PLACENTA ACCRETA. Prepared by : Dr . Amani A.A Rajab i , MD (AL_QUDS UNIV.) Resident at Makassed Islamic Charitable Hospital Supervised by : Dr . Saadeh S.Jaber MBBS, MRCOG, MRCPI, Head of OBGYN department Al_quds univ.

E N D
MAKASSED EXPERIENCE IN MANAGEMENT OF PLACENTA ACCRETA Prepared by : Dr . Amani A.A Rajabi , MD (AL_QUDS UNIV.) Resident at Makassed Islamic Charitable Hospital Supervised by : Dr . Saadeh S.Jaber MBBS, MRCOG, MRCPI, Head of OBGYN department Al_quds univ. Consultant at Makassed Islamic Charitable Hospital
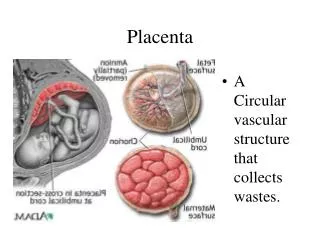
DEFINITION & PATHOGENESIS • Placenta accreta occurs when there is a defect of the decidua basalis , in conjunction with an imperfect development of the Nitabuch membrane , resulting in abnormally invasive implantation of the placenta . • Nitabuch membrane is a fibrinoid layer that separates the decidua basalis from the placental villi.
INCIDENCE • There is marked increase in the incidence of placenta accreta . • In 1950----- 1 in 30,000 deliveries . • In 1977-----1 in 7,000 deliveries . • In 1985-1994-----1 in 2500 deliveries . • In 1982-2002-----1 in533 deliveries . (Am J ObstetGynecol1997;177:210-4) (Am J Obstet and Gynecol (2005) 192, 1458–61)
placenta accreta has been reported to result in a 7% mortality rate . • The most common indication for birth related hysterectomy, accounting for 40–60% of cases. ACOG committee opinion . International Journal of Gynecology & Obstetrics 77 (2002) 77-78. J. Obstet. Gynaecol. Res. Vol. 33, No. 4: 431–437, August 2007 .
Color Doppler • Demonstrating turbulent flow through placental lacunae ,with abnormal vessels linking the placenta to the bladder.
Magnetic resonance imaging • The role of MRI is to complement, rather than replace, information obtained via standard sonographic imaging. • The main advantage offered by this type of imaging is : • The ability to diagnose posterior placenta accreta more confidently. • The assessment of bladder invasion in cases of placenta percreta.
The mean gestational age at diagnosis of placenta accreta by ultrasound is 29 weeks (range:28–33 weeks) . • The mean gestational age at delivery is 36 weeks (range: 32–38 weeks). J. Obstet. Gynaecol. Res. Vol. 33, No. 4: 431–437, August 2007 .
COMPLICATIONS • Massive obstetric hemorrhage is the most common complication . • Disseminated intravascular coagulopathy . • Adult respiratory distress syndrome . • Renal failure . • Infection • Death.
Abstract • STUDY DESIGN : Retrospective analysis of medical records & histopathological finding . • POPULATION : Women delivered at Makassed Hospital 2007 / 2008 of whom 15 cases of invasive placenta identified.A finding confirmed by histopathology . • METHODS : Retrospective analysis complemented with direct communication with patient ,using SPSS to analyze data . • CONCLISIONS : at the end of presentation .
Incidence in 2007 ….1:460 deliveries. • Incidence in 2008 ….1:300 deliveries. 9 6
Identified risk factorshistory of : • C S . • E &C . • IUCD . • Other uterine instrumentation .
Preoperative management • The woman should be informed of the diagnosis and potential complications . • Antenatal corticosteroid to be given . • Consent form of caesarean hysterectomy . • Delivery should be scheduled for optimal availability of necessary personnel and facilities. • A preoperative anaesthesia consultation should be obtained. • Adequate blood and clotting factors should be available at the time of delivery . • An intensive care unit should be available for postoperative care, as needed.
Immediate preoperative bilateral uretric stents were inserted in a couple of cases .
Intraoperative management of planned cesarean hysterectomy : • A vertical skin incision provides good exposure . • A vertical uterine incision is made above the upper edge of placenta . • Delivery of the baby . • Placenta left "in situ“, with minimal manipulation. • Extrafascial hysterectomy is then performed .
CONCLUSIONS • Incidence of invasive placenta at Makassed hospital is one case in 370 deliveries . • Invasive placenta associated with significantly high morbidity & mortality world wide , proudly the outcome in our hospital was excellent , with NO MORTALITY & MINIMUM MORBIDITY . • Excellent neonatal outcome .
Continued …. • Finally , maternal & neonatal outcome can be optimized by the availability of : • Senior obstetrician with advanced surgical skills . • Senior anesthesiologist & intensive care facilities . • Advanced lab & blood banking facilities . • Urological back up . • Intensive care baby unit .