Download

1 / 28
280 likes | 298 Views
This article explores the implementation of strategies relevant to national health care and specific centers in Central American and Caribbean countries. It discusses the health inequalities, disease prevalence, and lack of health care infrastructure in the region, while also highlighting the success of Cuba's National Health System and Chronic Renal Disease Program. The article emphasizes the importance of equity, prevention, and primary health care in improving the overall health outcomes in the region.

E N D
Implementation of Strategies Relevant to National Health Care and Specific Centers in the Emerging World: The View of Central American and Caribbean Countries Raúl Herrera-Valdés, MD, PhD Institute of Nephrology Havana – Cuba
Context of the Americas Mission: Promote equity in health, combat disease, and improve quality of life and life expectancy in the region. Health inequalities reflect socio-economic structural inequalities Values Equity – Excellence – Respect – Integrity
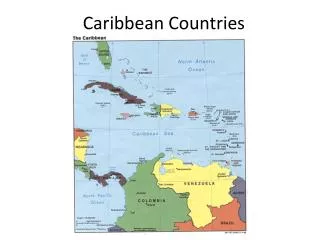
Central American and Caribbean Countries Wealthiest 20% 16 times INCOME 34 countries Population: 76 million Poverty: + 40% Countryside: 45% Poorest 20%
+ + - - - Stress Extreme living conditions Education Information Health Services Segregation Marginalization Poverty Disease
Illiteracy Latin Caribbean: 4%- 51% Central America5%- 36% Non- Latin Caribbean: 2%- 19%
Health Picture Communicable Diseases Non- Communicable Morbidity – Mortality Infant mortality rate: > 30 x 1,000 l.b. Life expectancy: < 70 years Infectious diseases Tendency Aging Non-Comm. Chr. Diseases
Health Picture: Risk factors for Renal Disease Near-poor population: Obesity epidemic Diabetes: 6% - 8%Hypertension: 8% - 30% Prevalence Increasing Ethnic Composition / Socio-economic conditions
Incidence & Prevalence of ESRD in RRT Incidence Prevalence Patients/MH Patients/MH País País Reg. L.A. de Diálisis y Trasplante.2001
Human Resources • Situation • Not enough professionals trained to meet health care needs. • Existing resources are inequitably distributed, concentrated mainly in the big cities. • Low salaries. • Internal and external migration. • Imbalance in the composition of healthcare workforce. • Minimal development of information resources. • Oriented towards curative care rather than prevention.
Physicians Latin Caribbean2.5 to 58.2 per 10,000 inh. Central America6.2 to 15 per 10,000 inh. Non-Latin Caribbean1.5 to 21.5 per 10,000 inh. • Nephrologists: • < 20 p.m.p in vast majority of countries • None in several non-Latin Caribbean nations
Health Care Infrastructure No preventive strategies in place for chronic renal insufficiency No institution which acts as a regional reference center
In the Central American and Caribbean context, Cuba shares many of the economic limitations of other countries, and at the same time, has advanced along the route of equity described by PAHO as critical to improving health in the region, as one of the countries with the least social disparity.
Cuba’s National Health System The health system is universal, public, and free-of-charge, with full coverage of the population. Cuba’s resource-scarce environment, coupled with public health principles, has reinforced a commitment to primary health care and prevention as the centerpiece of the system.
Health Care Situation in Cuba. Basic Indicators 2002 Total population 11.251 million Percent urban population 75.4% Literacy rate 96.2% Average educational level 9th grade Infant mortality rate ( x 1000 live births) 6.5 Life expentancy 76.15 Physicians per 10,000 population 59.6 Total number of family physicians 31,059 Population served by family physicians 99.2% Hospital beds ( x1000 population) 5.0
International Cooperation in Health (2003) Cuban health professionals serving abroad: 14,691 in 64 countries International medical students in Cuba: 9,023 from 83 countries
Cuban’s National Chronic Renal Disease Program: TRANSPLANTATION TERTIARY PREVENTION DIALYSIS ESRD CHRONIC RENAL INSUFFICIENCY CHRONIC RENAL DISEASES SECONDARY PREVENTION CLINICAL NEPHROLOGY HEALTHY POPULATION AND RISK GROUPS PRIMARY PREVENTION PRIMARY CARE: FAMILY DOCTORS
Cuban’s National Chronic Renal Disease Program:Organization and Resources NATIONAL COORDINATING CENTER NEPHROLOGY SERVICES: 34 OPENING: 13 100% Free Health Care PHYSICIANS: 67,000 FAMILY DOCTORS: 31,000 NEPHROLOGISTS: 385 Adult: 214 Pediatric: 66 Residents: 105 ORGAN PROCUREMENT CENTERS: 33 TISSUE TYPING LABORATORIES: 5 TRANSPLANTATION CENTERS: 9
National Chronic Renal Disease Program: Basic Indicators CRF patients HD Incidence RATE PMP 880 97.1 RATE PMP 1088 YEAR CRI Patients in follow-up * YEAR Trasplants Incidence HD Prevalence RATE PMP RATE PMP 134 19.5 YEAR YEAR
Prevention Program: Specific Objectives QUAL I TY OF L I FE Tertiary Prevention Secondary Prevention Primary Prevention
National CRD Program: Implementation of Prevention Strategies 47 Nephrology Services (Regions) 385 Nephrologists 444 Community Polyclinics ( Health Areas) 31 000 Family Physicians 99.2% Population
National CRD Program: Epidemiological Laboratory Isle of Youth 1 Municipal Health Service 1 Nephrology Service 5 Nephrologists 3 Community Polyclinics-Health Areas 105 Family Physicians 81,000 Persons Objective: Epidemiological follow-up for chronic renal diseases in total population by studying family units over time.
Community epidemiological laboratory for study of chronic renal disease (CRD). Isle of Youth project. Cuba. Control group CRD Cases Sample Total Cases Total population Phases of the project Actions Outcomes Screening • Dipstick for proteinuria • Short questionnaire Proteinuria (+) Proteinuria (-) CRD Diagnosis confirmation. Etiology. Dipstick for microalbuminuria in risk groups CRD Prevalence Proteinuria (-) Microalbuminuria (+) Microalbuminuria (-) Longer questionnaire Laboratory test Physical exam Case-control study Identify risk factors for CRD • CRD Incidence • CRD etiological risk factors • CRD progression Follow-up study Cohort Laboratory test Physical exam Cohort Preventive actions Therapeutic intervention • Risk reduction • CRD control Intervention Intervention • Morbidity patterns • Mortality tendencies • Distribution dialysis and • kidney transplant Surveillance Surveillance system
National CRD Program: National Coordinating Center Institute of Nephrology • Cuban School of Nephrology • National Reference Center • National Coordinating Center National Chronic Renal Disease Program Raising the Level of Medical Care Training Specialized Human Resources Developing Scientific Research • Management • Telenephrology • Epidemiological • Laboratory • Prevention • Clinical Nephrology • Dialysis • Transplantation
National CRD Program: Telenephrology Network XML Web services • National Institute of Nephrology • National Network of Nephrology Services. • National Health System’s National Telematics Network (INFOMED) • Second Opinion Services. • Teleconferencing. • Distance learning. • Epidemiological control (PC). • Selection of donor-recipient pairs. • CRI and Dialysis. • Statistics.
We place this modest Cuban experience at the disposal of our Central American and Caribbean colleagues and of nephrology societies internationally, inviting them to share with us their observations, reflections and expertise.
Conclusions • To prevent chronic renal disease in Central America and the Caribbean, we must: • Reduce poverty • Increase equity • Improve nutrition • Advance education • Develop health services • Formulate prevention policies • Create reference institutions
“These are dangerous times for the well-being of the world. In many regions, some of the most formidable enemies of health are joining forces with the allies of poverty to impose a double burden of disease, disability and premature death on many millions of people. It is time for us to close ranks against this growing threat. “ Gro Harlem Bruntland M.D.Director – General World Health Organization The World Health Report. WHO. 2002