Download
1 / 55
550 likes | 708 Views
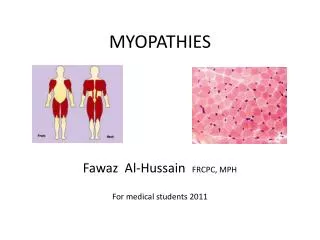
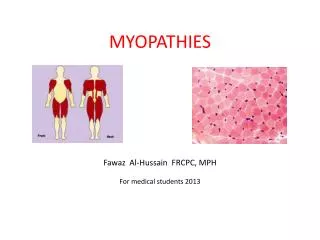
Recognition, Investigation and Treatment of Myopathies. Hanni Bouma August 14, 2013. Overview. Statin-induced myopathy Idiopathic inflammatory myopathies Dermatomyositis Polymyositis Inclusion body myositis. Etiological Classification of Myopathies. Hereditary Muscular Dystrophies

E N D
Recognition, Investigation and Treatment of Myopathies Hanni Bouma August 14, 2013
Overview Statin-induced myopathy Idiopathic inflammatory myopathies Dermatomyositis Polymyositis Inclusion body myositis
Etiological Classification of Myopathies Hereditary Muscular Dystrophies Duchenne’s Myotonias Channelopathies Congenital Myopathies Metabolic Myopathies Pompe’s disease Mitochondrial myopathies Acquired Inflammatory myopathies PM, DM, IBM Endocrine thyroid Associated with other systemic illness Drug-induced and toxic myopathies EtOH, steroids, statins
Statin-induced Myopathy • 1.5-3% of statin users in RCTs and 10-13% of participants enrolled in prospective clinical studies develop myalgias; rates of myositis lower (~0.1-0.5%) & dose-dependent • Mean duration of statin therapy before onset of Sx.: 6 months • Mean duration of myalgias after stopping statin therapy: 2 months
Questions • What if a patient develops a myopathy after several years of taking a statin? • Are some statins more likely to cause muscle damage? Which ones?
Management • Significant muscle Sx.: discontinue statin • Asymptomatic but with CK>10x ULN: discontinue statin • Rhabdo: no statins at any time due to risk of recurrence • If requires a statin but muscle toxicity other than rhabdo: discontinue statin • Once Sx. have resolved and the CK has returned to baseline, can try pravastatin or fluvastatin with careful monitoring
Questions • When are EMG or muscle biopsy necessary in suspected statin myopathy? • Is Coenzyme Q10 helpful?
Statin-associated necrotizing myopathy • Myopathy which persists or progresses after stopping statin • Linked to autoantibodies against HMG-CoA reductase • Distinct muscle biopsy findings: • macrophagocytic infiltrate engulfing necrotic muscle fibers • Responds to immune therapy
DM: Clinical Slow, progressive, symmetric limb-girdle weakness Activity-induced muscle pain Rash usually accompanies or precedes weakness (but not always) Associated features: Adults: Myocarditis, ILD, vasculitis, other CTDs (RA, Scl, CREST) Children: Contractures, subQ calcinosis, intestinal ulceration Malignancy: adenocarcinomas, ovarian, breast, lung, lymphoma/leukemia
DM: Investigations CK normal (20-30%) or increased up to 50x ANA+ (24-60%) Myositis specific antibodies: Mi-2 (15%) acute onset, nailfold ulcers & good response to therapy Anti-Jo-1 (~20%) ILD, mechanic’s hands, arthritis, Raynaud’s EMG Muscle biopsy MRI
Other Investigations: DM Increased risk of Ca. within first 2-3 yrs of diagnosis Treatment of malignancy sometimes improves muscle strength Malignancy workup in all patients: CT CAP Mammogram Breast & pelvic exams Colonoscopy And/OR PET scan CXR, High res CT chest (ILD) EKG (myocardial inv’t) or Echo if CHF Swallowing assessment if dysphagia
Polymyositis “Diagnosis of exclusion” Often mistaken diagnosis of PM in cases of DM w/o rash (yet) or IBM w/o inclusions on biopsy Adults with prox symmetric weakness: limb girdle distribution + neck flexors Also ass’d with other autoimmune disorders Myocarditis, arthritis, Raynaud’s, ILD
IBM Most common myopathy > 50 yo Insidious onset; Dx. usually several yrs after onset Early dysphagia Different pattern of weakness: Distal UE, Prox LE Early atrophy & weakness of WF, FF & quads Hip girdle, TA muscles
EMG findings(all IM) • Fibs, PSWs, CRDs at rest • Increased insertional activity
Why fibs? 1) Distal, healthy portion of muscle fibre gets separated from the part attached to the endplate 2) Infarction of small intramuscular nerve twigs by surrounding interstitial inflammation
EMG findings • Polyphasic, low amplitude, short duration MUPs with voluntary activation • Rapid recruitment of MUPs w/ full interference pattern of low amplitude on weak effort
PM Mediated by CD8+ T-cells which attack muscle fibres Endomysial mononuclear inflammatory cell infiltrate invading and surrounding non-necrotic muscle fibres
DM Humorally-mediated microangiopathy • Perifascicular necrosis/atrophy • Perivascular & perimysial inflammation: • macrophages, B cells, CD4+ cells
IBM Similar to PM: CD8+ T cells & macrophages Modified Gomori trichrome stain Same features as PM + rimmed vacuoles + amyloid deposits
Is it possible to have IBM without inclusions on biopsy? Question
MRI • DM: inflammation mainly in anterior muscle compartments • w/ preserved muscle mass • PM/IBM: fatty infiltration/muscle atrophy in all muscle groups
Treatment of DM & PM Overall lack of “EBM” to guide treatment; we don’t know: Which second linetherapies are most beneficial The doses required to see an effect The best time to initiate 2nd or 3rd line agents If some agents are more effective in certain types of myositis
Treatment: Step 1Initiate corticosteroids Treatment of choice in DM & PM: Majority of patients will improve with pred, but response may be incomplete Start prednisone at ~1 mg/kg/day up to 100 mg qd In severe weakness, treatment often initiated w/ short course of IV Solumedrol 1 g x 3 days prior to pred
Treatment: Step 1Post-initiation of steroids Close clinical F/U q2-4 weeks initially Maintain dose until muscle strength normalizes, improvement plateaus, or CK normalizes (at least 4-6 wks at high dose) Then slow taper: by 5 mg q2-3 weeks, below 20 mg by 2.5 q2wks
Treatment: Step 1Side effect considerations for steroids Monitor fasting glucose, K+ levels Septra for PCP prophylaxis If concurrent ILD or pred + other immunosuppressant Bone density scan at baseline & qyearly Calcium 1 g/day + Vit D 1000 IU/day Bisphosphonate used if postmenopausal Record BP at each visit (accelerated HTN & renal failure is a risk) Coexistence of scleroderma & other MCTDs Periodic eye exams for glaucoma & cataracts
Question What should I do if there is no response after an adequate trial of high dose prednisone?
Question How can I tell if the patient is weaker because of refractory disease or because of chronic steroid use?
Treatment: Step 2Add immunosuppressant Indications: Moderate or severe weakness Other organ system inv’t (ILD, myocarditis) Increased risk of steroid complications (diabetic, OP, postmenopausal women) Failure to significantly improve after 2-4 months of steroids Any pt expected to need steroids for 10-12 mos or more
Treatment: Step 2Immunosuppression Options: Azathioprine Methotrexate IVIG Cellcept Cyclophosphamide Generally used as 3rd line, if refractory to other Rx.: Rituximab PLEX Ciclosporine Tacrolimus
Azathioprine Effective in DM/PM (retrospective studies), but takes 6-18 mos to work Prior to starting, can screen for TPMT deficiency (BM toxicity in homozygotes) or just monitor CBC Begin at 50 mg/d, increase by 50 mg q2wks up to 2-3 mg/kg/d
AzathioprineMonitoring & SEs Major SEs: 12% develop systemic rxn (fever, abdo pain, N/V) within first few wks requiring discontinuation of drug; BM & liver toxicity, pancreatitis, teratogenicity, oncogenicity, infection Leukopenia Monitor CBC, LFTs closely
Methotrexate Most DM & PM respond to MTX (retrospective studies only) Begin at 7.5 mg/wk po, increase gradually by 2.5 mg each week up to 25 mg/wk If no improvement after 1 month on 25 mg, switch to weekly subQ & increase dose by 5 mg qwk up to 60 mg/wk
MethotrexateMonitoring & SEs Major SEs: alopecia, stomatitis, pulmonary fibrosis, teratogenicity, oncogenicity, infection; renal, liver & BM toxicity Avoid MTX in pts with ILD or anti-Jo-1+ Avoid MTX in heavy drinkers Treat all pts with folate 5 mg qwk
IVIG One prospective, double-blind, placebo-controlled study in 15 pts w/ DM showed significant improvement Little RCTevidence of benefit as monotherapy but plenty of anecdotal evidence that IVIG is effective, even alone
Cyclophosphamide • Used often if ILD • SEs: infections, secondary malignancies, hemorrhagic cystitis, sterilization, BM toxicity, GI upset, alopecia • Usually given pulsed; higher risk of cystitis po
Treatment: Step 3If refractory to other modalities… Rituximab -> monoclonal Ab against CD20, depletes B cells Warnings re: PML risk…
Non-medical therapies PT & OT Dietician consult if on steroids Aerobic exercise programs Prevents contractures May help w/ steroid SEs (weight gain, OP, type 2 fibre atrophy) Speech therapy Esp if concomitant dysphagia
Question What is the value of monitoring serum CK levels in the treatment of DM & PM?