Download
1 / 26
260 likes | 373 Views
Level of HIV-1 unspliced RNA in PBMC: a longitudinal marker of infection progression in untreated individuals and a predictive marker of virological rebound in patients on ART with undetectable plasma viremia. Alexander Pasternak Laboratory of Experimental Virology

E N D
Level of HIV-1 unspliced RNA in PBMC: a longitudinal marker of infection progression in untreated individuals and a predictive marker of virological rebound in patients on ART with undetectable plasma viremia Alexander Pasternak Laboratory of Experimental Virology Department of Medical Microbiology Academic Medical Center University of Amsterdam Amsterdam, The Netherlands XVIII International AIDS Conference, July 22, 2010
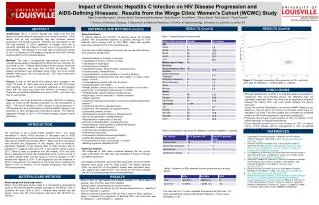
PCR II (real-time, 40-45 c) PCR II (real-time, 40-45 c) PCR I (conventional, 15 c) PCR I (conventional, 15 c) Development of sensitive seminested real-time PCR methods tat gag vif nef 5’LTR vpu 3’LTR rev pol vpr env prDNA, usRNA msRNA usRNA, prDNA msRNA
Pre-amplification results in 3-4 log stronger input signal Proviral DNA Unspliced RNA 3.5 log 3.75 log Multiply spliced RNA Seminested real-time PCR Single-step real-time PCR 4.25 log
Sensitivity is increased 1.5 log without losing the linearity Proviral DNA Unspliced RNA 1.5 log 1.5 log Multiply spliced RNA Seminested real-time PCR Single-step real-time PCR 1.5 log
prDNA 100% 94% usRNA 100% 94% msRNA 83% 16% PBMC were isolated at baseline and at multiple time points during therapy cART failures (n=15) HIV-1 plasma load successes (n=11) 50 copies/ml start of cART
P=0.002 P=0.001 P=0.008 Longitudinal trends of virological parameters and CD4+ count in patients on cART
P=0.002 P=0.006 P=0.001 P=0.32 P=0.008 P=0.005 Longitudinal trends of virological parameters and CD4+ count in patients on cART
Pdiff = 0.56 Pdiff = 0.64 Pdiff = 0.73 Pdiff = 0.02 Levels of virological parameters and CD4+ count in patients on cART future failures (n=15) successes (n=11)
Pdiff = 0.24 Pdiff = 0.15 Pdiff = 0.0015 Levels of virological parameters and CD4+ count in patients on cART future failures (n=15) successes (n=11)
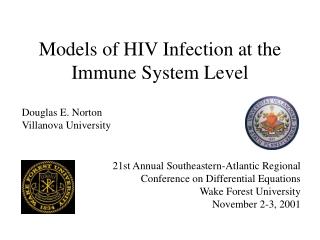
P=0.0033 (univariate) P=0.024 (multivariate) 1 14 future failures 7 4 successes The risk of virological rebound according to the maximal usRNA value during cART Risk of VR, % Maximal usRNA level during cART, log10 copies/µg total RNA
rs = 0.74; P < 0.0001 rs = 0.16; P = 0.45 rs= -0.56; P = 0.003 rs = -0.65; P = 0.0003 Correlations of virological parameters and CD4+ count
Conclusions (I) Levels of usRNA in PBMC in patients on cART with undetectable plasma viremia are strongly predictive of the subsequent outcome of therapy. Levels of prDNA gradually diminished during the therapy period in both patient groups, whereas levels of usRNA dropped sharply after the start of therapy, but subsequently reached the plateau, with the difference between the usRNA levels of future cART failures and successes established early after the start of cART and persisting throughout the therapy period. Levels of usRNA under cART strongly inversely correlated with baseline CD4+ count, but did not correlate with either baseline usRNA levels or prDNA levels under therapy. The observation that patients with higher levels of usRNA in PBMC were more prone to failing cART might link higher cellular HIV-1 RNA load in these patients with virus replication under therapy, which resulted in selection of drug-resistance mutations.
Longitudinal trends of plasma HIV-1 RNA are highly variable between patients No reliable longitudinal virological markers of HIV-1 infection progression in the asymptomatic phase are known => How about untreated patients?
How about untreated patients? To compare the dynamics of HIV-1 molecular markers in PBMC and plasma in untreated infection, we selected 10 untreated patients and measured HIV-1 usRNA, msRNA, and prDNA levels at multiple time points during the asymptomatic phase (clinical latency)
Longitudinal slopes Time-weighted changes from baseline ns ns ns ns ns ** * ** * ** ** ** ** ** * * ** ** Changes from baseline ns ns ns ns ** ** ** ** Longitudinal trends of the analyzed parameters
Longitudinal trends of the analyzed parameters: linear mixed model
rs = 0.13 Correlations between the virological parameters and CD4+ count rs = -0.43 rs = -0.46
Conclusions (II) Levels of HIV-1 RNA and DNA in PBMC increased during the asymptomatic phase of infection in untreated individuals with stable RNA levels in plasma. Levels of usRNA increased faster than those of prDNA: an increase in viral replication rates in PBMC. Levels of usRNA and prDNA, but not those of plasma RNA, inversely correlated with CD4+ count, which is itself a marker of infection progression in the asymptomatic phase. Level of usRNA in PBMC (which was shown earlier to be a predictive marker of the response to cART) is also a longitudinal marker of infection progression in the asymptomatic phase of the untreated infection.
Acknowledgements Karen Adema Margreet Bakker Marion Cornelissen Joke Brouwer Suzanne Jurriaans Ben Berkhout Vladimir Lukashov Medical Microbiology, Academic Medical Center of the University of Amsterdam, The Netherlands Jan Prins Internal Diseases – Infectious Diseases, Tropical Medicine and AIDS, AMC, UvA This study was financially supported by Dutch AIDS Fonds, project nr. 2004045
The problem is simple… virological rebound, drug-resistant viruses HIV-1 plasma load detection limit start of cART
virological failure, drug-resistant viruses HIV-1 plasma load detection limit start of cART The problem is simple…
Longitudinal trends of plasma HIV-1 RNA are highly variable between patients No reliable longitudinal virological markers of HIV-1 infection progression in the asymptomatic phase are known Henrard et al., JAMA, 1995 De Wolf et al., AIDS, 1997 => Geskus et al., Retrovirology, 2007 Korenromp et al., PLoS ONE, 2009 How about untreated patients?
Correlations between the virological parameters rs = 0.69 rs = 0.46 rs = 0.42
Differences in longitudinal trends between prDNA and usRNA can be explained by the fact that prDNA levels reflect the size of the proviral archive, whereas levels of usRNA reflect the amounts of productively infected cells at every moment in time. The observed difference in the usRNA levels between failures and successes may be shaped by the difference in the relative amounts of latently infected resting CD4+ T cells that become reactivated to the productively infected phenotype and escape immunological clearance. The observed difference in the usRNA levels between failures and successes may be shaped by the difference in the relative amounts of latently infected resting CD4+ T cells that become reactivated to the productively infected phenotype and escape immunological clearance. The relative amount of productively infected cells at any moment during cART (reflected in the usRNA level) might be defined, to a large extent, by the immunological state of the patient before therapy (reflected in the CD4+ count), and not simply by the size of viral reservoir (reflected in the levels of prDNA). The relative amount of productively infected cells at any moment during cART (reflected in the usRNA level) might be defined, to a large extent, by the immunological state of the patient before therapy (reflected in the CD4+ count), and not simply by the size of viral reservoir (reflected in the levels of prDNA). The observation that patients with higher levels of usRNA in PBMC were more prone to failing cART might link higher cellular HIV-1 RNA load in these patients with virus replication under therapy, which resulted in selection of drug-resistance mutations. Discussion (I) Differences in longitudinal trends between prDNA and usRNA can be explained by the fact that prDNA levels reflect the size of the proviral archive, whereas levels of usRNA reflect the amounts of productively infected cells at every moment in time.
Discussion (II) So why is the increase in viral replication in PBMC is not (or, not significantly) paralleled by an increase in plasma viremia? Plasma HIV-1 load reflects the balance between the virus production and clearance, whereas the cellular HIV-1 load would reflect the virus production only. It is possible that the ability of the immune system to clear free virus is compromised during the asymptomatic phase to a lesser extent than the ability to clear HIV-infected cells. During this phase of infection, the weakening immune system may still possess a capacity to adjust the virus clearance rates to the increased virus production; when this capacity is exhausted, the uncontrolled virus replication rapidly leads to the onset of AIDS. Alternatively, because most HIV-1 replication takes place in the lymphoid tissue, the virus produced by the infected PBMC may not substantially contribute to the total amount of free virus found in plasma.