Download
1 / 74
1.15k likes | 2.21k Views
Yıldırım Beyazıt University Medical Faculty Biochemistry Department. Lipoproteins. Prof. Dr. Fatma Meriç YILMAZ fatmamericyilmaz@hotmail.com. Lipids in the Blood. Fatty Acids Bound to albumin. Cholesterol, Triglycerides and Phospholipids Transported by lipoproteins

E N D
Yıldırım Beyazıt University Medical Faculty Biochemistry Department Lipoproteins Prof. Dr. Fatma Meriç YILMAZ fatmamericyilmaz@hotmail.com
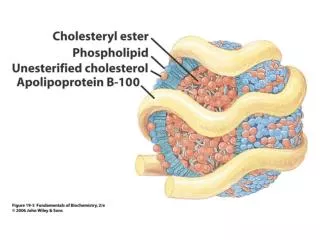
Lipids in the Blood • Fatty Acids • Bound to albumin • Cholesterol, Triglycerides and Phospholipids • Transported by lipoproteins • Cholesterol can be free or esterified
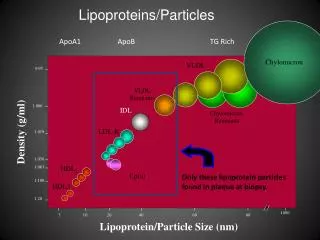
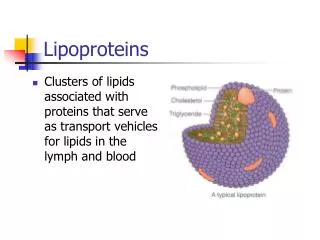
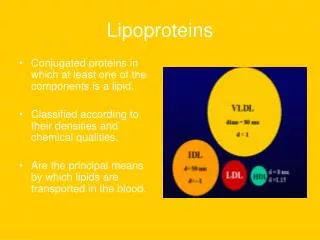
Lipoproteins • particles found in plasma that transport lipids including cholesterol • lipoprotein classes:
Lipoproteins • Chylomicrons are the LP particles lowest in density and largest in size (Contain highest percentage of lipids and lowest percentage of proteins) • IDLs and LDLs are denser, having higher ratios of protein to lipid • HDLs are the densest LP particles with the highest protein contents
Apolipoproteins • Structural determinants of lipoproteins • Enzyme cofactors • Ligands for binding to lipoprotein receptors
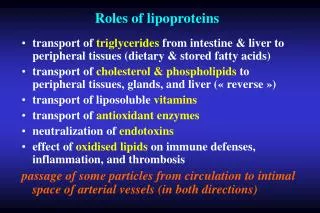
Functions of Apolipoproteins Provide recognition sites for cell-surface receptors Serve as activators or coenzymes for enzymes involved in lipoprotein metabolism Some of lipoproteins are essential structural components and cannot be removed Some of them are transferred freely between lipoproteins Apolipoproteins are divided into five groups by structure and function (A to E) Most classes have subclasses like Apo A-I, Apo C-II etc. Functions of all apolipoproteins are not yet known
apoA-I HDL structural protein; LCAT activator;RCT apoA-II Hepatic Lipase activation apoA-IV Tg metabolism; LCAT activator; dietresponse apoB-100 Structural protein of all LP except HDL Binding to LDL receptor apoB-48 apoC-I Inhibit Lp binding to LDL R; LCAT activator apoC-II LpL activator apoC-III LpL inhibitor; antagonizes apoE apoE B/E receptor ligand Apolipoproteins
Enzymes and Transfer Proteins • LCAT(Lecithin:CholesterolAcyltransferase) • Formation of cholesterol esters in lipoproteins (HDL) • ACAT(Acyl-CoA:CholesterolAcyltransferase) • Formation of cholesterol esters in cells • CETP(Cholesterol Ester Transfer Protein) • Transfer of CE from HDL to VLDL and • transfer of TG from VLDL to HDL
Chylomicrons • particles consisting of phospholipids, Chol/CE triacylglycerols and apolipoproteins • Apolipoproteins (Apo B48, Apo CII, Apo E)
Chylomicrons Chylomicrons are synthesized in intestinal epithelial cells, secreted into the lymph, pass into the blood, andbecome mature chylomicrons On capillary walls in adipose tissue and muscle, lipoprotein lipase (LPL) activated by ApoCIIdigests the triacylglycerols (TG) of chylomicrons to fatty acids and glycerol. Fatty acids (FA) are oxidized in muscle or stored in adipose cellsas triacylglycerols. The remnants of the chylomicrons are taken up by the liver by receptor-mediated endocytosis (Apo E receptors). Lysosomal enzymes within thehepatocyte digest the remnants, releasing the amino acids, free cholesterol and fatty acidsinto the cytosol.
ChylomicronCirculation Apo-B48 is uniquetochylomicrons Theparticlereleasedfromintestinalcellsarenamed as nascent CM andcarriesonlyApo B48 When it reachestotheplasma is has beenmodified; Apo C II andApo E particlesaretransferredfromHDL Apo C II activates LPL enzyme As thechylomicroncirculates, morethan 90% of TG in itscore is degradedby LPL, theparticledecreases in size, increases in density C apoproteinsreturnto HDL andtheparticle is called a remnant CM Remnant CM stillcontainsApo E andbindstotheliverthroughApo E receptors
CII E B48 B48 Mature CM CM Remnant CII AI Nascent CM FFA E FFA Glycerol FFA FFA HDL LPL TISSUE Blood Vessel Intestine
E CII B48 HDL AI LIVER CM Remnants are taken to the liver and hydrolized Apo E receptor
VeryLowDensityLipoproteins (VLDL) VLDLs are produced in the liver They are composed of predominantly of endogeneous triacylglycerol (60%) The main function of VLDL is to carry this lipid from the liver to the peripheral tissues The TG of VLDL, produced in the liver, isdigested by lipoprotein lipase (LPL) present on the lining cells of the capillaries in adiposeand skeletal muscle tissue. Fatty acids are released and either oxidized or stored in tissues asTG.
VLDL Circulation VLDL is secreteddirectlyintothebloodbytheliver as nascent VLDL particlescontainingApo B-100 TheymustobtainApo C-II andApo Efromcirculating HDL Apo C-II activates LPL and as VLDL passthroughthecirculation, TGsaredegradedbylipoproteinlipase, causing VLDL todecrease in size andbecomedenser Surfacecomponents, includingthe C and E apoproteinsarereturnedto HDL but theparticlesretainApo B-100 Finallysome TG aretransferredto HDL andcholesterolestersaretransferredfrom HDL to VLDL withCholesterol Ester Transfer Protein (CETP) Withthesemodifications, VLDL is convertedto LDL in theplasma
Role of CETP in Triglyceride/Cholesteryl Ester Exchange VLDL LDL TG TG HDL HDL CETP CETP CE CE
IntermediateDensityLipoprotein (IDL) Intermediate-density lipoproteins are formed from the degradation of VLDLs Some of the IDL particles are rapidly taken up by the liver through Apo E receptors; others remain in circulation, where they undergo further triglyceride hydrolysis and are converted to LDL Carry Apo E and Apo B-100
LowDensityLipoprotein (LDL) LDL particles contain much less TG then their precursor VLDL and have a high concentration of cholesterol and cholesteryl esters The primary function of LDL is to provide cholesterol to peripheral tissues LDL particles contain Apo B100 which is the receptor binding site for LDL particles These receptors can also bind Apo E and are named as Apo B100/Apo E receptors
B100 E CII B100 Mature VLDL CII AI E Glycerol HDL FFA FFA FFA FFA LPL TISSUE Nascent VLDL Blood Vessel
E CII HDL B100 ApoD AI LDL KARACİĞER LDL is taken up with LDL receptors Apo B100 receptors
HighDensityLipoprotein (HDL) HDL comprise a heterogeneous family of lipoproteins with a complex metabolism that is not completely understood. HDL is a reservoir of apolipoproteins Apo C-II and Apo E HDL takes up the cholesterol esters from peripheral tissues and returns it to the liver It is responsible from esterification of cholesterol with LCAT enzyme
HighDensityLipoprotein (HDL) Nascent HDL are disk shaped particles containing primarily phospholipid and Apo A, C and E They take up cholesterol from peripheral tissues and return it to liver as CE. When chol is taken up by HDL, it is immediately esterified with LCAT LCAT enzyme is synthesized by the liver. LCAT binds to nascent HDL and is activated by Apo A-I
HighDensityLipoprotein (HDL) LCAT transfersthefattyacidfromcarbon 2 of phosphotidylcholintocholesterol Thisproduces a hydrophobiccholesteryl ester which is transferredtothecore of thelipoprotein As thediscoidalnascent HDL accumulatescholesterylesters, it firstbecomes a spherical, relativelycholesteryl ester poorHDL3 thenturnstoHDL2 which is cholesteryl ester rich HDL form.
HDL Metabolism KC Apoproteins HDL HDL receptor mediated endocytosis in liver HDL HDL Transfer of some CE To VLDL (CETP) “used” cholesterol is Transferred to HDL and converted to cholesteryl esters (LCAT) VLDL Cholesterol is secreted to bile or repackaged to form VLDL LDLreceptor mediated endocytosis Peripherictissues LDL LDL
Lipoprotein(a), or Lp(a) • An atherogenic lipoproteincontaining apo(a) and apoB. • 20-30% of people have levelssuggesting CV risk. • Black subjects have Lp(a)normal range twice as highas white and Asiatic subjects. • Apo(a) sequence similar to plasminogen, and Lp(a)interferes with spontaneous thrombolysis. • Lp(a) levels highly genetic, resistant to diet and drugtherapy. Apo(a) “LDL” -S-S-
The function of the heart is to circulate blood throughout the body by: • Pumping blood through the lungs removes carbon dioxide and refreshes the blood with oxygen • The oxygenated blood is pumped to the body to provide oxygen and nutrients and to remove waste products. • The coronary arteries are the blood vessels that supply blood and oxygen to the heart muscle.
Atherosclerosiscan, and does, occur in almost any artery in the body. But in the heart it’s effects can be crucial. • The body depends on a strong pumping heart to circulate life-giving blood, and this includes to the heart muscle itself. • If the coronary arteries become blocked, the cardiac muscle begins to fail, and so the blood circulation decreases, which includes the circulation to the heart muscle itself.
Clinical Manifestations of Atherosclerosis • Coronary heart disease • Stable angina, acute myocardial infarction, sudden death, unstable angina • Cerebrovascular disease • Stroke, TIAs • Peripheral arterial disease • Intermittent claudication, increased risk of death from heart attack and stroke American Heart Association, 2000.
“OLD THEORY” • High cholesterol causes plaque by building up on wall of arteries—therefore, focus was on lowering cholesterol as much as possible BUT…. • 1) In 10 year study period on island of Crete, there were no recorded heart attacks despite high cholesterols • 2) French study showed reduced risk of second heart attack or cardiac-related death in those following the “Mediterranean Diet” compared to those on a low fat “cardiac” diet, despite similar cholesterol levels in both groups
“NEW” THEORY • Atherosclerosis is the result of damage to the endothelium (inner lining of arteries) and inflammation causing progressive damage • This then allows cholesterol (especially “oxidized” LDL) to enter the artery wall-causing more damage and reaction from the immune system-builds plaque • Creates cycle of inflammation and plaque • Progressively narrows the artery and it becomes stiffer, interfering with blood to vital organs
Pathology and pathogenesis • The lesions associated with atherosclerosis are of three types: • The fatty streak • The fibrous atheromatous plaque • Complicatedlesion • The latter two are responsible for the clinicallysignificant manifestations of the disease.
Mechanisms • There is increasing evidence that atherosclerosis is at leastpartially the result of: • (1) endothelial injury with leukocyte(lymphocyte and monocyte) adhesion and platelet adherence • (2) smooth muscle cell emigration and proliferation • (3) lipid depositionof activated macrophages • (4) subsequent developmentof an atherosclerotic plaque with lipid core
Mechanisms • One hypothesis of plaque formation suggests that injury to the endothelial vessel layer is the initiating factor in the development of atherosclerosis. • Possible injurious agents are: • Products associated with smoking; • Immune mechanisms; • Mechanical stress, such as that associated with hypertension. • Hyperlipidemia, particularly LDL with its high cholesterol content, is also believed to play an active role in the pathogenesis of the atherosclerotic lesion.
LDL – cholesterolandAtherosclerosis • The LDLis removed from the circulation by either LDL receptors or byscavenger cells such as monocytes or macrophages. • Approximately70% of LDL is removed by way of the LDL receptordependentpathway. • Although LDL receptors are widely distributed,approximately 75% are located on hepatocytes; thusthe liver plays an extremely important role in LDL metabolism. • Tissues with LDL receptors can control their cholesterol intakeby adding or removing LDL receptors.
LDL – cholesterolandAtherosclerosis • The scavenger cells, such as the monocytes and macrophages,have receptors that bind LDL that has been oxidized orchemically modified. • Theuptake of LDL by macrophages in the arterial wall can result inthe accumulation of insoluble cholesterol esters, the formationof foam cells, and the development of atherosclerosis.
Mechanisms of Atherosclerosis • One of the earliest responses to endothelial disfunction is the attachment of monocytes to theendothelium. • The monocytes emigratethrough the cell-to-cell attachments of the endothelial layerinto the subendothelial spaces, where they are transformedinto macrophages. • Activated macrophages release free radicalsthat oxidize LDL. • Oxidized LDL is not recognized at the cell receptor level and so, it can not be internalized and it longer remains into the blood stream.
Endothelial disruption leads to platelet adhesionand aggregation and fibrin deposition. • Platelets and activatedmacrophages release various factors that are thought to promotegrowth factors that modulate the proliferation of smoothmuscle cells and deposition of extracellular matrix in the lesions: elastin, collagen, proteoglycans. • Activated macrophages also ingest oxidized LDL to becomefoam cells, which are present in all stages of atheroscleroticplaque formation. • Lipids released from necrotic foamcells accumulate to form the lipid core of unstable plaques. • Connective tissue synthesis determinates stiffness, calcium fixation and further ulceration of atheromatous plaque.
Modern theory of atherosclerosis • Multifactor theory: • Structural and functional injury of vascular endothelium; • Response to injury of immune cells and smooth muscle cells; • The role of lipoproteins in initiation and progression of lesions; • The role of growth factors and cytokines; • The role of repeated thrombosis in lesions progression.
Hyperlipidemias It is also known as hyperlipidemia or hyperlipoproteinemia It is defined as a presence of raised or abnormal levels of lipids and/or lipoproteins in the blood This abnormality is common in the general population, and is one of the important modifiable risk factors for coronary heart disease (CHD). Dyslipidemia is generally characterized by increased fasting concentrations of total cholesterol (TC), LDL cholesterol (LDL-C), and triglycerides (TG), in conjunction with decreased concentrations of HDL cholesterol (HDL-C)
Hereditary Hyperlipoproteinemias • On diagnosing hyperlipoproteinemia, hyperlipidemic status should be evaluated to determine whether it is primary lipoprotein disorder or secondary to any of a variety of metabolic diseases. • The diagnosis of primaryhyperlipoproteinemia is made after secondary causes have been excluded. • Primary hyperlipoproteinemias are genetic disorders and classified from I to V
Type I Hyperlipoproteinemia • Familial Lipoprotein lipase deficiency • Characterized by high levels of chylomicrons and triglycerides and a deficiency of lipoprotein lipase • Disease onset is usually in infancy. • Type 1 has a pure elevation of triglycerides in the chylomicron fraction.These people sometimes getpancreatitisand abdominal pains, but they do not seem to have an increase in vascular disease.
Type II Familial hypecholesterolemia • Type II, broken into two subtypes, type II-a and type II-b. • Type II a. LDL Receptor/Apo B 100 deficiency • Type II b. Increased production of Apo B • The familial (genetic) versions of Type II often develop xanthomas, which are yellow fatty deposits under the skin of the knuckles, elbows, buttocks or heels. They may also have xanthelasmas, smaller yellow patches on the eyelids. Both subtypes display high levels of blood cholesterol. People with type II-b also have high levels of triglycerides in their blood. Disease onset is usually after age 20.