Download
1 / 79
860 likes | 1.31k Views
ICM II: Shoulder and Hand. Scott Pollock, MD Clinical Professor of Medicine Division of Rheumatology. Outline. Introduction Shoulder Anatomy review Three common problems and one you shouldn’t forget Hand/wrist Anatomy review Three common problems and one you shouldn’t forget

E N D
ICM II: Shoulder and Hand Scott Pollock, MD Clinical Professor of Medicine Division of Rheumatology
Outline • Introduction • Shoulder • Anatomy review • Three common problems and one you shouldn’t forget • Hand/wrist • Anatomy review • Three common problems and one you shouldn’t forget • Conclusion
Introduction • Developing a diagnosis Working diagnosis Lab and X-rays 1-2 possibilities Physical Exam 1-3 possibilities Patient History 2-4 possibilities
Introduction • Before you can ask the right questions you need to know the potential answers • Experience is a great teacher • Physicians catalog knowledge based on the patients and patient problems they have encountered • When you are on the your clinical rotations, try to be involved with as many patients as you can. • An experienced clinician actually has fewer Differential Diagnoses (DDx) than a less experienced clinician
Introduction • When unsure about your examination think about what structures are in the area that might be causing problems • Bones/joints • Arteries/veins • Nerves • Muscles • Tendons/ligaments • Skin/fascia/lymph nodes • Most patients do not need a complete exam, they need an exam based on your differential; good to learn a complete exam so you can know which examination parts to perform
Introduction Basic MS physical examination pieces Stability and Provocative Tests Strength Testing Range of Motion (active and passive) Palpate • ICM • Please • Remember (I’m a) • Second (year) • Student Inspect (examine both sides)
Inspection Look from front, back and side Compare symptomatic side to normal Look for known anatomic structures: bones, muscles Look for deformities, signs of inflammation and swelling
Palpation Have a systematic approach to each region/joint Bones, joints, tendons, bursae, muscles Compare any abnormalities to the contralateral side Approach known painful areas carefully and gently, palpating non-painful first (you can really cause pain)
Range of Motion Observe patient during history; how symmetrically do they move the symptomatic region? Test active ROM first with a functional test If this is abnormal (limited, painful, distorted), then test passive ROM (if passive ROM painful, joint pathology) Know what normal ROM is supposed to be
In the human body, which are the most incredible joints? • Back • Knee • Hand • Shoulder • None of the above
Shoulder Anatomy Examination Approach to the patient with shoulder pain: clinical cases
Shoulder • Second most common location for musculoskeletal complaints • Difficult joint to examine • Multidirectional range of motion- UNIQUE! • Shoulder injury can affect nearly every sport and many daily activities and all ages
Evolution The shoulder must be mobile enough for the wide range actions of the arms and hands, but also stable enough to allow for actions such as lifting, pushing and pulling. The compromise between mobility and stability results in a large number of shoulder problems not faced by other joints such as the hip.
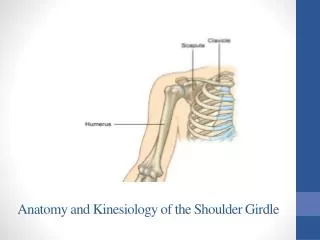
Glenohumeral Joint • Shallow (“golf ball sitting on a tee”) • Inherently unstable (maximizes ROM) • Static stabilizers • glenohumeral ligaments, glenoid labrum and capsule • Dynamic stabilizers • Predominantly rotator cuff muscles • Also scapular stabilizers • Trapezius, levator scapulae, serratus anterior, rhomboids
Deltoid Rotator cuff Teres major Latissimusdorsi Biceps Pectoralis muscles Other Anatomy
Physical Exam • Inspection • Palpation • Range of Motion • Strength • Neurovascular • Special Tests
Physical Exam Observe the patient front/side/back, noting posture Compare shoulders (deformity, atrophy, difference in height, bony prominences) Perform exam systematically Patient demographics and history guide exam Is shoulder real cause of pain or is it referred from: cervical spine, gall bladder, spleen, heart, etc.
Physical Exam: Inspection Front, side & back Height of shoulder and scapulae Muscle atrophy, asymmetry Compare both sides
Palpation Cervical spine Scapula: spine, bony edges, adjacent musculature Acromion and subacromial space Bicipital groove and greater/lesser tuberosities Clavicle, including SC and AC joints
Physical Exam: Range of Motion Evaluate 4 sites of motion:SternoclavicularAcromioclavicularGlenohumeral (30/12)Scapulothoracic Active vs. Passive ROM
Physical Exam: Range of Motion Abduction 0-180o
Physical Exam: Range of Motion • Forward flexion: • 0o – 180o
Physical Exam: Range of Motion • Extension • 0o – 40 to 60o
Physical Exam: Range of Motion • Internal rotation • T5 segment • External rotation • 80-90o
Shoulder ROM: Apley Scratch Tests A: adduction; B: external rotation and abduction; C: internal rotation and adduction
Special Tests Impingement Rotator Cuff Integrity Labrum and Biceps AC (SC) Joints Instability
Shoulder pain isn’t always from the shoulder!!Get more history… • Gall bladder or liver disease • Peptic Ulcer Disease • Cervical radiculopathy • Cardiac ischemia • Pulmonary conditions • i.e. Pancoast’s tumor, Pneumonia
Red Flags for Shoulder Pain • When to think infection/tumor • Age over 50 • Fever/chills/weight loss • History of cancer • Recent IV drug use • Crescendo pain • Can’t find a comfortable position at night • Sudden onset shoulder pain, marked severity • Calcific tendinopathy • Acute intra-abdominal process • Fracture, possibly pathologic (neoplasm)
Case #1: Shoulder pain • 45 year old man comes into clinic for evaluation of R shoulder pain • Hx of increased overhead work under car preceeding pain • No hx of fall or other trauma • 2 months reduced ROM R shoulder, pain reaching forward or above his head, impaired sleep due to pain • Denies neck pain, parasthesias/numbness into R arm • ROS is entirely negative for heart, lung, GI disorders
Differential Dx at this Point Subacromial bursitis Bicipital tendonitis Rotator cuff tendonitis (supraspinatus, etc.) Rotator cuff tendon tear Osteoarthritis of glenohumeral joint Cervical disc disease RUQ abdominal disease (e.g. gall stones, other) Pulmonary process
Case #1: Examination • Inspection: holds arm at side (adducted), difficulty undressing, no erythema or swelling • Palpation: tenderness anteriorly (not clearly over biceps tendon) & laterally in the subacromial region • ROM: reduced active abduction due to pain, pain with Apley Scratch Tests (IR, ER, abd/extension), passive ROM—pain past 90 degrees abduction, but others full • Strength: probably normal, but pain and guarding limit accuracy • Normal ROM neck without pain, normal neuro/abd/lung exams
Differential Dx after Exam Subacromial bursitis Bicipital tendonitis Rotator cuff tendonitis (supraspinatus, etc.) Rotator cuff tendon tear Osteoarthritis of glenohumeral joint Cervical disc disease RUQ abdominal disease (e.g. gall stones, other)
Subacromial bursitis Case #1: Shoulder pain Deltoid Subacromialsubdeltoid bursa Biceps tendon Fluid Steroid injection cured Humerus
Case #2: Shoulder Pain 75 yo woman complains of 3 wks of L shoulder pain She fell 1 day before the pain began, landing on her L shoulder with arm outstretched and thigh Did not see MD Pain at rest, at night and with any movement shoulder Trouble getting dressed
Differential Dx at this Point Subacromial bursitis Bicipital tendonitis Rotator cuff tendonitis (supraspinatus, etc.) Rotator cuff tendon tear Osteoarthritis of glenohumeral joint Humeral fracture Cervical disc disease RUQ abdominal disease (e.g. gall stones, other) Pulmonary process
Case #2: Shoulder pain--exam Inspection: fading bruise over anterolateral, anterior swelling L shoulder Palpation: bogginess, tender over anterolateral ROM: can not move actively in any direction due to pain and guarding; passive ROM slightly better but hurts at 50% of usual Strength: very weak, pain limits testing Neuro: decreased ROM neck without pain, normal sensory exam and DTRs upper extremities
Differential Dx Subacromial bursitis Bicipital tendonitis Rotator cuff tendonitis (supraspinatus, etc.) Rotator cuff tendon tear Osteoarthritis of glenohumeral joint Humeral fracture Cervical disc disease RUQ abdominal disease (e.g. gall stones, other) Pulmonary process
Case #2: Shoulder pain Massive rotator cuff tear
Case #3: Shoulder pain 80 yo woman comes in to the clinic with complaint of slowly progressive pain and limited mobility of R shoulder No hx of falls, trauma, overuse Hurts to dress, to lie on shoulder at night She has osteoarthritis of hands and a hx of L total hip replacement for OA hip Past medical hx: hypothyroid, angina/CAD stable
Differential Dx at this Point Subacromial bursitis Rotator cuff tendonitis (supraspinatus, etc.) Rotator cuff tendon tear Osteoarthritis of glenohumeral joint Humeral fracture Cervical disc disease RUQ abdominal disease (e.g. gall stones, other) Pulmonary process Coronary artery disease
Case #3: Shoulder pain—exam Elderly woman in NAD No asymmetry of shoulders, no erythema or swelling, mild deltoid muscle atrophy Mild diffuse tenderness over all aspects of shoulder Marked loss of motion of R shoulder in all directions with moderate pain Mild decrease ROM neck Normal neuro exam
Differential Dx Subacromial bursitis Bicipital tendonitis Rotator cuff tendonitis (supraspinatus, etc.) Rotator cuff tendon tear Osteoarthritis of glenohumeral joint Humeral fracture—pathologic Cervical disc disease RUQ abdominal disease (e.g. gall stones, other) Coronary artery disease
Case #3: Shoulder pain Severe OA right shoulder with massive rotator cuff tear Referral to orthopedist for possible shoulder replacement
Case #4: Shoulder pain 65 yo man brought into ER with L shoulder and upper arm pain of 3 hour duration Pain began while asleep, does not vary with deep breathing or position Mild sweating (diaphoresis) and jaw ache No hx of trauma or overuse No numbness, burning or weakness in L arm Medical hx: hypertension, diabetes mellitus