Download
1 / 19
250 likes | 1.82k Views
The Shoulder: Positioning and Handling Considerations Post-Stroke. 11 December 2008 Sonja Findlater Occupational Therapist sfindlater@dthr.ab.ca. Learning Goals. Upon completion of the session, the participants will be able to:

E N D
The Shoulder: Positioning and Handling Considerations Post-Stroke • 11 December 2008 • Sonja Findlater • Occupational Therapist • sfindlater@dthr.ab.ca
Learning Goals • Upon completion of the session, the participants will be able to: • Provide a rationale for encouraging the client to participate in moving the more-affected limb. • Make some basic alignment adaptations to encourage use of the hemiparetic arm. • Describe a common cause of hemiparetic shoulder pain. • List some strategies to prevent/minimize shoulder pain. • Position and support the hemiparetic arm.
Fill in the Blanks • HANDLING CONSIDERATIONS: • 1) ___________________________________________________ • 2) ___________________________________________________ • 3) ___________________________________________________ • 4) ___________________________________________________ • POSITIONING CONSIDERATIONS: • 1) ___________________________________________________ • 2) ___________________________________________________ • 3) ___________________________________________________
Background • Incidence of Shoulder Pain Post CVA • Effects: Increased LOS, Decreased Quality of Life, Decreased Independence with ADL’s • Preventable? • It takes a village…
Key Concept Body Schema • “Through the integration of proprioceptive, tactile, and pressure input, the body scheme becomes the neural foundation for perception of body position and the relationship of the body and its parts.” • (van Deusen in Zoltan, 2007) • Handling Consideration: Tactile and proprioceptive information to the more-affected limb contributes to body schema!
Key Concept Alignment • Falling • Neurologically, ‘falling’ occurs when our COM (centre of mass) goes beyond our stability limits. Therefore, our system may feel that we are ‘falling’ even if we are in bed, a chair etc. • The vestibular system receives afferent information from the semicircular canals, the visual system, the cerebellum and spinal cord. Activation of this system results in antigravity muscle activity. (Latash, 2008) • TASK: what does vestibular activity look like?? • POSITIONING CONSIDERATION: Position to prevent excessive vestibular activity • Optimal Alignment • The cerebellum notes change in alignment - this input updates our body schema. Potentiation of activity. • HANDLING CONSIDERATION: Align a limb so that it MAY be able to move
Key ConceptPostural Control • Postural Control • Proximal stability to enhance distal mobility • “Good” and “bad” sides after a stroke - not so black and white! (Gillen, 2004) (Kandell, 2000) • Anticipatory Postural Adjustments • APA’s prepare the body for the expected pertebation of a voluntary movement. • APA’s are FEEDFORWARD, not feedback • APA’s are learned • HANDLING CONSIDERATIONS: Encourage the person to HELP you move their limb/let them KNOW that you are going to move their limb!!
Resting Position of the Scapula: Gillen, 2004 pg. 205
Scapular Motions Elevation/Depression (Lippert) Abd/Adduction (Lippert) Up/Downward Rotation (Lippert) Movements Not Pictured: Int/External Rotation & Ant/Posterior Tipping
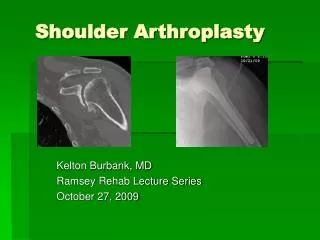
Scapulohumeral Rhythm • ref: Neumann, 2002 pg 126 & 115
Shoulder Pain Prevention • Maintain glenohumeral external rotation • Maintain scapular mobility on the thorax • Avoid passive or active shoulder movements beyond 90 degrees unless the scapula is gliding toward upward rotation and sufficient external rotation is available. • Educate!!!! • Positioning - ax shoulder positions in bed, wheelchair and during upright function • Avoid activities that may cause impingement such as pulleys. • (Gillen, 2004 pg. 204) • Handling Consideration: As the humerus approaches 90 degrees of flexion or abduction, it needs to externally rotate and the scapula needs to upwardly rotate
Positioning • Bed • Head/Neck = symmetrical • Affected UL = protracted scapula, supported UL, wrist & fingers extended • Trunk = aligned • Affected LL = flexed and supported. • Positioning Consideration: Scapular protraction & Supported humerus
Positioning • Wheelchair • Head/Neck = symmetrical • Affected UL = protracted scapula, supported UL, wrist & fingers extended • Trunk = aligned • Affected LL = supported... FOOTRESTS!!!! • Eating
Shoulder Supports • Red Flag • Shoulder Supports • Slings • Trays • “... if the goal of treatment is to provide glenohumeral joint stability, then the device must support the scapula on the ribcage with the glenoid fossa facing upward, forward, and outward and must compensate for a lack of support by the rotator cuff and possibly the superior capsule.” (Gillen, 2004 pg. 209)
Annotated Bibliography Etc.... • Neurology Texts • Latash, ML. Neurophysiological Basis of Movement. 2nd ed. Champagne, IL: Human Kinetics, 2008. Kandel ER, Schwartz JH, Jessell TM. Principles of Neural Science 4th ed., 2000, McGraw-Hill. • Websites • Evidence Based Review of Stroke Rehabilitation www.ebrsr.com • APSS www.strokstrategy.ab.ca • Stroke Engine www.medicine.mcgill.ca • Anticipatory Postural Adjustments • APA’s were reduced in individuals with hemiparesis. The results suggest that the ability of individuals with hemiparesis to prepare for a self-initiated predictable perturbation is reduced and that they may use alternative strategies of stabilization. (Slijer, 2002) • Reduced APA activity was found in the studied trunk muscles (lat dorsi, ext oblique, rectus abdominis) on the paretic side of the body. Erector Spinae were the least affected of the monitored muscles. (Dickstein, 2004) • Trunk Muscle Activity Post Stroke • Bilateral Trunk Rotation Weakness Post Stroke. In stroke subjects – rotated just as well to each side, despite side of hemiparesis. HOWEVER, this muscle performance was decreased to both sides when compared to healthy subjects. The author hypothesized that this finding may be due to descending bilateral innervation of the trunk muscles. (Tanaka, 1997) • Differential Activation in Symmetrical versus Asymmetrical Tasks. Similar Rectus Abdominis activation on affected and non-affected sides during symmetrical activity, lower output of RA in asymmetrical activity (shoe donning) (Winzeler-Mercay, 2002) • Horak study: hemiplegic subjects demonstrated same sequence of muscle activation as subjects without hemiplegia, although activity was delayed. Also, the hemiplegic subjects were unable to make rapid movements with the unimpaired arm (Gillen, 2004)
References • Dickstein R, Shefi S, Marcovitz E, Villa Y. Anticipatory postural adjustments in selected trunk muscles in poststroke hemiparetic patients. Archives of Physical Medicine and Rehabilitation 85(2004) 261-267. • Gillen G, Burkhardt A. Stroke Rehabilitation, A Function Based Approach 2nd ed., St. Louis, 2004, Mosby. • Kandel ER, Schwartz JH, Jessell TM. Principles of Neural Science 4th ed., 2000, McGraw-Hill. • Latash, ML. Neurophysiological Basis of Movement. 2nd ed. Champagne, IL: Human Kinetics, 2008. • Levangie PK, Norkin CC. Joint Structure and Function: A Comprehensive Analysis. Philadelphia, 2005, F.A. Davis Company. • Lippert L. Clinical Kinesiology for Physical Therapist Assistants, Philadelphia, 1994, F.A. Davis Company. • Neumann DA. Kinesiology of the Musculoskeletal System, Foundations for Physical Rehabilitation. St. Louis, 2002, Mosby. • Slijer H, Latash ML, Rao N, Aruin A. Task specific modulation of anticipatory postural adjustments in individuals with hemiparesis. Clinical Neurophysiology 113 (2002) 642-655. • Tanaka S, Hachisuka K, Ogata H. Trunk rotary muscle performance in post-stroke hemiplegic patients, Am J Phys Med Rehabil 1997; 76(5): 366-369. • Winzeler-Mercay U, Mudie H. The nature of the effects of stroke on trunk flexor and extensor muscles during work and at rest. Disability and Rehabilitation. 2002:24(17): 875-886. • Zoltan B. Vision, Perception, and Cognition, A manual for the evaluation and treatment of the adult with acquired brain injury. 4th ed. New Jersey 2007, Slack Inc.