Download
1 / 65
660 likes | 966 Views
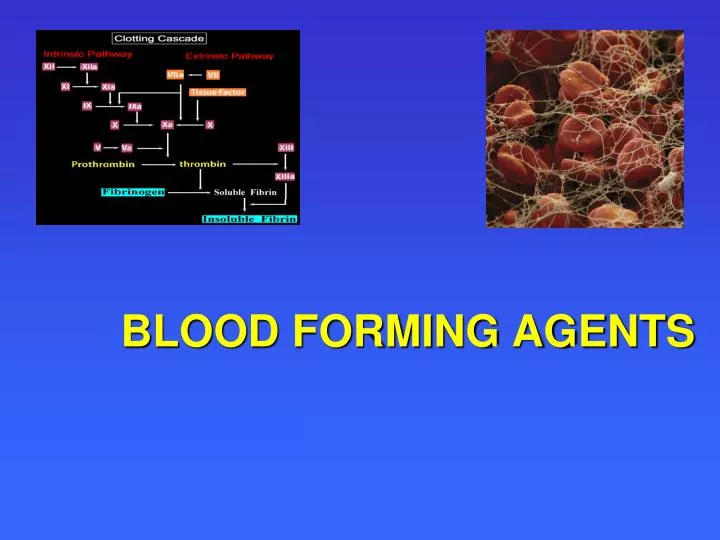
BLOOD FORMING AGENTS. Clinical Thrombosis. > 2.5 million cases of deep venous thrombosis (DVT) annually > 600.000 cases of pulmonary embolism (PE) per year > 50.000 deaths per year from PE > 11.000 post surgical PE deaths per year. Anti Platelet Drugs. INHIBITORS OF PLATELET AGGREGATION.

E N D
Clinical Thrombosis • > 2.5 million cases of deep venous thrombosis (DVT) annually • > 600.000 cases of pulmonary embolism (PE) per year • > 50.000 deaths per year from PE • > 11.000 post surgical PE deaths per year
Platelets inhibitors - ASA Kardiomagnil Daily dose - 80-100 mg
ANTIPLATELET THERAPYAspirin Indications 1) Stroke, TIA (transient ischemic attacks) 2) MI, recurrent MI 3) Unstable angina 4) CABG potency (coronary artery bypass graft)
TICLOPIDINE 1) Interferes with platelet-fibrinogen binding 2) Exerts its action for the life of the platelet 3) May prolong bleeding time • Useful for coronary artery stents and CVA (cerebrovascular accident) 5) Methylprednisolone may reverse its effect 6) Associated with TTP (thrombocytopenic purpura), neutropenia, and diarrhea
CLOPIDOGREL • Interferes with GP IIb/IIIa • (Glycoprotein IIb/ IIIa) binding site • 2) Exerts its action for the life of the platelet • 3) May prolong bleeding time • 4) Indicated for prevention of MI, CVA (cerebrovascular accident), and vascular death • 5) Fewer side effects than ticlopidine • 6) Dose: 75 mg daily
Abciximab (ReoPro) • Human-mouse monoclonal antibodies • Binds to GP (glycoprotein) IIb/IIIa receptor on platelets • Half-life 10 min. • May block receptor for 10 days • Indicated for prevention of closure of coronary vessels after angioplasty • May cause thrombocytopenia • Used with heparin and ASA
Mechanism of heparin action 5 АТ ІІІ ІІ а 5 АТ ІІІ Х а 10 13 АТ ІІІ – ant thrombin ІІІ ІІ а – thrombin Х а – prothrombinase (Stuart-Proverfactor)
HEPARIN IV or SC administration only
HEPARIN (Indications) Full Dose:5000 U or 80 U/kg IV bolus, followed by 1200-1600 U/hr adjusted to therapeutic range 1) Acute deep venous thrombosis 2) Pulmonary emboli 3) Unstable angina and myocardial infarction Low Dose:5000 U sq q12 h 1) Postoperative prophylaxis of any major abdominal, thoracic, gynecologic, or orthopedic procedure 2) Immobilized medical patients >40 yrs. with CHF, CVA, malignant disease 3) Prophylaxis for underlying hypercoagulable state Other Dose: 1) Extracorporeal bypass 2) Hemodialysis 3) After thrombolytic therapy
HEPARIN (Contraindications) 1) Thrombocytopenia 2) Aspirin or alcohol use 3) Hepatic or renal disease 4) Other platelet dysfunction 5) GI bleeding 6) Tumors
HEPARIN (Side Effects) 1) Major side effect is bleeding 2) Osteoporosis with prolonged use 3) Thrombocytopenia w
HEPARIN-INDUCED THROMBOCYTOPENIA 1) Occurs in 2-5% of patients receiving standard heparin by immune mechanism • May occur with minute doses, including heparin flushes • More common with bovine than porcine heparin • Asymptomatic thrombocytopenia can occur in 30-50% of pts who develop HIT antibodies • ~20-50% of thrombocytopenic patients develop arterial or venous thrombosis that may be life threatening
HEPARIN-INDUCED THROMBOCYTOPENIA Alternative Anticoagulants- direct thrombin inhibitors • Lepirudin • Argatroban
LOW MOLECULAR WEIGHT HEPARIN 1) Molecular weight 3,000- 7,000 D 2) Inhibits factor Xa rather than thrombin 3) Factor Xa assay used for monitoring 4) Administered subcutaneously 2 times/d 5) Probably less antigenic than standard heparin 6) Recommended for prophylaxis and treatment
LOW MOLECULAR WEIGHT HEPARIN 1) PT, APTT not usually prolonged 2) May be monitored with anti-factor Xa assay
jjjjjjjjjjjjjjjjjjjjjjjjjjjjjjjjjjjjjjjjjjjjjjjjjjjjjjjjjjjjjjjjjjjjjjjjjjjjjjjjjjjjjjjjjjjjjjjjjjjjjjjjjjjjjjjjjjjjjjjjjjjjjjjjjjjjjjjjjjjjjjjjjjjjjjjjjjjjjjjjjjjjjjjjjjjjjjjjjjjjjjjjjjjjjjjjjjjjjjjjjjjjjjjjjjjjjjjjjjjjjjjj
LOW MOLECULAR WEIGHT HEPARINS ggggggggggggggggggg
Indications for and Contraindications to Parenteral Anticoagulant Agents
Heparin-Antibiotic Interactions • The cephalosporins- cefamandole, cefotetan, and cefoperazone, contain an N-methylthiotetrazole (NMTT) side chain. This NMTT group can: • - Dissociate from the parent antibiotic in solution or in vivo and competitively inhibit vitamin K action, leading to prolongation of the prothrombin time and bleeding. • - This side chain is also associated with a disulfiram-like reaction to alcohol.
ANTICOAGULANTS OF INDIRECT ACTIONCOUMARIN (Description) 1) Isolated by Link in 1939 after previous observation that cattle developed bleeding disorder after ingestion of spoiled clover 2) Is 4-hydroxycoumarin compound, similar in structure to vitamin K 3) Administered p.o., rapid GI absorption 4) Crosses placenta easily (complications!) 5) Interacts with a variety of drugs
COUMARIN (Actions) 1) Blocks the carboxylation of the vitamin K dependent clotting proteins, factors II, VII, IX, and X, maintaining them in their inactive forms 2) Blocks the anticoagulant proteins C and S 3) Onset – 18-48 hours
COUMARIN Laboratory 1) Prolongs the PT and APTT 2) PT and Prothrombin index -used for monitoring
Prothrombin indexINTERNATIONAL NORMALIZED RATIO (INR) INR = PATIENT PT CONTROL PT Decrease no less than 50 %
COUMARIN Side Effects 1)Hemorrhage 2) Fetal abnormalities 3) Skin necrosis with deficiencies of proteins C or S usually on 3rd to 8th day of therapy
COUMARINInteractions POTENTIATORS : Phenylbutazone Cimetidine Omeprazole Amiodarone Anabolic steroids ANTAGONISTS : Barbiturates Rifampin Penicillins Antacids