Download
1 / 52
530 likes | 580 Views
Learn about pressure ulcers: stages, risk factors, prevention methods, and complications. Understand skin layers, factors causing ulcers, risk assessment scales, and preventive strategies. Comprehensive resource.

E N D
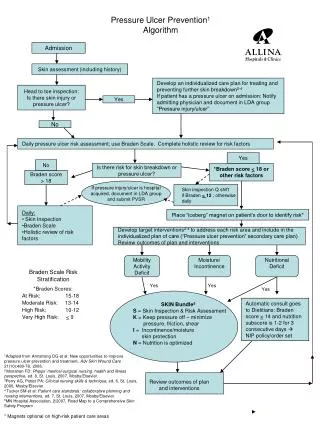
Pressure Ulcer Prevention and Management DiptiJethani RN BSN Alverno College All motion clips/images not labeled obtained from Microsoft Clip Art
Navigation NEXT SLIDE PREVIOUS SLIDE HOME /TABLE OF CONTENTS LAST SLIDE VIEWED
Learning Objectives • Learner will be able to identify the stages of pressure ulcers • Learner will be able to identify patients at risk for pressure ulcers • Learner will be able to identify 3 ways to decrease risk and incidence of pressure ulcers • Learner will be able to identify 3 complications of pressure ulcers
Let’s Start With A Case Study • Grace is an 84 year old female who was recently admitted into the hospital with a diagnosis of Pneumonia. • She has been weak, she used a cane before admittance in the hospital. She now is only mobile per wheel chair. • She also is an uncontrolled Type II Diabetic (Non-Insulin Dependent) • HOW WILL YOU PREVENT HER FROM DEVELOPING PRESSURE ULCERS? Doheny, Patrick. (2007). Happy planet one. [Photograph]. Retrieved fromhttp://www.flickr.com/photos/14132971@N05/1449122304/.
What Factor Most Puts Grace at Risk for Pressure Ulcers? • Age • Lack of Mobility • Diabetes • Having Pneumonia • Having a cane – she’ll beat the nurses up! Click Here To Read Case Study Narrative
THE SKIN • Three Layers • Epidermis • Outermost Layer • Contains sensory receptors for pain, temp, touch, vibration, and pressure detection • Barrier to preserve moisture, vitamins, minerals, and proteins • Dermis • Lies beneath the epidermis, deeper and thicker too • Contains connective tissue, & sebaceous glands • Contains fat &sweat glands • Subcutaneous Tissue • Layer of fat and connective tissue • Layer of insulation to conserve body heat National Pressure Ulcer Advisory Panel (2007). For Educational Purposes. Lippincott Williams and Wilkins, 2011
Let’s Review… What are pressure ulcers?? • Also known as: Pressure/Bed Sores • Areas of cellular necrosis and skin breakdown most common over bony prominences • Can occur anywhere on the body • Most Common Sites: Sacrum, Heels http://www.nlm.nih.gov/medlineplus/ency/imagepages/19091.htm For Educational Purposes, NIH Lippincott Williams and Wilkins, 2011
Incidence of Pressure Ulcers Estimated: 1 mill/yr; annual cost = $1.6 billion The elderly account for > 60% of decubitus patients Since 2008, hospitals are not able to be reimbursed for the care of Stage III or IV pressure ulcers that the patient acquires during their hospital stay 63% increase in hospitalized patients with pressure ulcers between 1993 and 2003 There has been no sig decrease in pressure ulcers in the last 10 years Most often seen in elderly Bedridden; Chair Bound 9 out of 10 patients were covered by a government program (Medicare or Medicaid) In 2007, CMS reported 257,412 cases of preventable pressure ulcers as secondary diagnoses Anders, 2010; Sage Products Inc (2003) Mereck Manual of Geriatrics, 2000; Krasner (2008).
Risk Factors • Extrinsic Factors • Pressure • Friction • Shearing • Intrinsic Factors • Immobility • Inactivity • Incontinence • Malnutrition • Age • Mental Status Mereck Manual of Geriatrics, 2000
Assessing the Risk • BEGINS ON ADMISSION • Skin Exam • On admission and every shift • History of Pressure ulcers • Recent weight loss • Mobility Status • Urinary/Bowel Incontinence • Dietary Intake/Nutr Status • Use Scales For Assessment • Braden Scale • Norton Scale • PUSH Tool Guren, D., 2010.
Used to accurately predict who will develop pressure ulcers • 6 Areas of Assessment: Sensory Perception, Activity, Mobility, Skin Moisture, Nutritional Intake, Friction and Shear Braden Scale • Scored from 1-4 • 1 for low level of functioning and 4 for the highest level or no impairment • Total scores range from 6-23 • At Risk (15-18) • Moderate Risk (13-14) • High Risk (10-12) • Very High Risk (9 or below) Cassell, 2009.
Prevention • BEGINS AT FIRST CONTACT • Turn patient at least every 2 hours • Do not place pts in a 90 degree lateral position • Puts more pressure on greater trochanter and lateral malleolus • Don’t elevate HOB > 30 degrees (except when eating) to minimize shearing forces • Avoid Fluorescent Light, it casts a blue tint to skin (Capezuti, 2008) • Check skin of high risk patients for changes in: • Color, turgor, temp, and sensation. Mereck Manual of Geriatrics, 2000
Prevention Cont. • Patient should not sit more than 2 hours • Sitting position puts increased pressure on ischial tuberosities. • Reposition patient every hour in chair • Teach patient to shift weight every 15 minutes • Do not use pillows/ rubber doughnuts • Keep skin surface clean and dry (Meticulous skin care) • As few pads as possible should be used • Main Points: • Keep pressure off the area of breakdown • Clean and dress the wound • Maintain good nutrition Mereck Manual of Geriatrics, 2000
Prevention • Monitor Lab Values: • HgB <12 • Total Lymphocyte Count <1200 • Serum Albumin <3.5 • Serum Transferrin <170 • Promote Movement and Freq Position Changes (Anders, 2010) Mereck Manual of Geriatrics, 2000
Pressure Relief Aids Lippincott Williams and Wilkins, 2011
Pressure Points • Most Develop Over 5 locations: • Sacral Area • Greater Trochanter • Ischial Tuberosity • Heels • Lateral Malleolus • 90% occur in lower body Agency for Health Care Policy and Research (2008) Lippincott Williams and Wilkins, 2011; Abrass, 2004
Case Study • Grace has a history of COPD and has smoked 1 PPD for 22 years, but quit 7 years ago. • Her Diabetes has progressed and due to complications her Left foot was amputated. • On the last shift a small Stage I pressure ulcer was also discovered.
What complication should the nurse most focus on preventing? A. Progression of the Ulcer to a new stage B. Increased Length of Stay C. Infection D. Sepsis E. All of the Above F. A and B only Click Here To Read Case Study Narrative
Stages of Pressure Ulcers • 6 Stages • Staged according to depth of damage Bright Hub Inc, 2011. Public Domain Image Mereck Manual of Geriatrics, 2000
Suspected Deep Tissue Injury • Maroon or purple intact skin or a blood filled blister • Cause: shearing or pressure on the underlying soft tissue • Before discoloration occurs, the area may be: • Painful • Mushy, firm, or boggy • Warmer or cooler as compared to other tissue National Pressure Ulcer Advisory Panel (2007). For Educational Purposes. Abrass, 2004
Stage I • An area of intact skin that does not blanch and is usually over a bony prominence. • NON-BLANCHABLE • Darkly pigmented skin may not show blanching but its color may differ from the surrounding area. • The area may be painful, firm or soft, or warmer or cooler when compared to the surrounding tissue. National Pressure Ulcer Advisory Panel (2007). For Educational Purposes. Abrass, 2004
Stage II • A superficial partial thickness wound • Presents as a shallow, open ulcer without slough and with a red and pink wound bed. • This term shouldn’t be used to describe: • Perineal dermatitis, maceration, tape burns, skin tears or excoriation . • Only use to describe • An abrasion, a blister, or a shallow crater that involves the epidermis and dermis. National Pressure Ulcer Advisory Panel (2007). For Educational Purposes. Abrass, 2004
Stage III • A full-thickness wound with tissue loss. • The subcutaneous tissue may be visible but muscle, tendon, or bone is not exposed. • Slough may be present but it does not hide the depth of the tissue loss. • Undermining and tunneling may be present. • Bone/Tendon are NOT visible National Pressure Ulcer Advisory Panel (2007). For Educational Purposes. Abrass, 2004; NPUAP, 2007
Stage IV • Involves Full-Thickness skin loss • Can visibly see exposed muscle, bone, or tendon • Eschar and sloughing may be present as well as undermining and tunneling National Pressure Ulcer Advisory Panel (2007). For Educational Purposes. Abrass, 2004
Unstageable • Involves full-thickness tissue loss. • The base of the ulcer is covered by : • Slough: yellow, tan, gray, green, or brown OR • Eschar: tan, brown, or black • The pressure ulcer cannot be staged until enough eschar or slough is removed to expose the base of the wound National Pressure Ulcer Advisory Panel (2007). For Educational Purposes. Abrass, 2004
Definitions • Friction: Surface damage caused by skin rubbing against • another surface. • Shearing: Trauma to skin caused by tissue layers sliding against each other, results in disruption of blood vessels. • Maceration: Softening of tissue by soaking in fluids. • Debridement: Removal of damaged tissue. • Eschar: Thick, leathery necrotic tissue; damaged tissue. • Slough: Loose, stringy necrotic tissue • Undermining: Tissue destruction underlying intact skin • along wound edges. • Tunneling: A narrow channel/passageway extending into • healthy tissue. Oklahoma Foundation for Medical Quality, 2009
Case Study Cont. • Which of the following is Grace most at risk for? • Friction • Shearing • Maceration • Laceration Click Here To Read Case Study Narrative
Case Study Click Here To Read Case Study Narrative • Grace became incontinent of bowel and bladder. • She has a decreased appetite and has become more confused since the last shift. • A urine specimen was obtained and results show she has a UTI.
What measures can you take to prevent progression and development of pressure ulcers?
Pathophysiology Affected area becomes hypoxic and ischemic d/t press exerted on it Decreased blood flow to site Capillaries Collapse, Thrombosis occurs Tissue Edema/Necrosis Accumulation of waste products at site Tissue Breakdown Cell Death Lippincott Williams and Wilkins, 2011
Stress Response and Pressure Ulcers Stress occurs Adrenal Glands produce Epi SNS releases NE NE causes peripheral vasoconstriction Decreased Oxygen Delivery Epi enhances production ofchalone Chalone protein depresses regeneration of epidermal tissue Tissue Breakdown Cell Death Epi = Epinephrine NE = Norepinephrine Place mouse over chalone to see definition Maklebust, J., & Sieggreen, M. (2001).
Aging • Muscle & fat are lost with aging (to spread out press) • Skin Elasticity Decreases • in ascorbic acid levels: • BVs & Connective tx more fragile • Lowers threshold of pressure injury • in # of Dermal BVs: • Incr risk of ischemic injury by press and shearing forces • Wound healing ed: • Repair rate declines • Cell proliferation es • Wound tensile strength es • Collagen deposition es Lippincott Williams and Wilkins, 2011; Mereck Manual of Geriatrics, 2000
Inflammation Damaged BVs Exposed Collagen With Thrombin exposed collagen stimulates platelet activity Activation, aggregation, and adhesion of platelets and release mediators Stimulates Vasoactive substances Breakdown products attract nuetrophils and macrophages Monocytes become Macrophages Release growth factors Trigger Fibroblasts to secrete collagen & proteins Wound becomes beefy red and bleeds Vasculature begins to restore Hulse, 2011
Genetics • Study by Bregstorm & Braden (2002) • found A.A. lowest risk for Stage I ulcers & Caucasians at highest risk for developing Stage I ulcer • For stages II-IV AA most at risk for progression of an ulcer & Caucasians least at risk • Certain Medical Conditions • Diabetes M. • Peripheral Vascular Dx • Predisposed to developing pressure sores Capezuti, 2008 Mereck Manual of Geriatrics, 2000
Pressure Ulcers on Heels • Account for 20% of all pressure ulcers • Easy to acquire hard to heal • Pressure relief • Pillows (floating) • Heel Protector Boots • Dressing if necessary • Foam Pads Guren, D., 2010.
Complications • Progression of pressure ulcer • Secondary Infections • Ex. Sepsis, Cellulitis • Osteomyelitis Loss of limb from bone involvement • Marjolin’s Ulcer • Squamous cell carcinoma within the ulcer • Increased Length of Stay • Increased Costs • Death Lippincott Williams and Wilkins, 2011 Mereck Manual of Geriatrics, 2000; Capezuti, 2008
Treatment • Prevention Strategies • Pressure Reduction • Avoiding Friction/ Shearing Forces • Stage III/IV • Debridement of necrotic tissue • Freq Irrigation (2-3x/d) • Dressing of the wound • Encourage movement Abrass, 2004; Anders, 2010
POP QUIZ Identify the pressure ulcer stage of the following area of skin abnormality . Public Domain Image obtained from: http://i.ytimg.com/vi/QvcjH98ipeU/2.jpg
IF YOU SAID: STAGE III YOU WERE RIGHT!!
Nutrition • Need adequate intake for wound healing and immune response • Incr protein/caloric intake • Supplement with multi-vitamins (A & C) • Consult with a Dietician • Loss of > 15% of lean body mass interferes with wound healing • Immune Function Loss • => Incr risk of infection and decr wound healing Anders, 2010; Maklebust, J., 2001
Nursing Implications Krasner, 2008
Documentation • Location • Size • Dressing • Type of irrigation soln, drsg applied • Drainage • Amt, color, odor • Undermining/Tunneling Present • Infection s/s • Character of wound • Presence of slough, granulation tissue, etc • Pressure relieving measures used Hill Rom Services Inc., 2007
CASE STUDY CONT. • What aspect of Grace’s existing condition is the most influencing factor for increasing her risk for pressure ulcers? • Pneumonia/COPD • Diabetes • Venous Insufficiency • Lack of Mobility • None of the Above • All of the Above Click Here To Read Case Study Narrative
Case Study Conclusions • Press ulcers can increase morbidity and risk for complications • Grace represents a typical patient • Documentation and thorough assessment is a necessity • FOR A VIRTUAL TOUR OF SKIN BREAKDOWN SEE NEXT SLIDE Doheny, Patrick. (2007). Happy planet one. [Photograph]. Retrieved fromhttp://www.flickr.com/photos/14132971@N05/ 1449122304/.
http://www.youtube.com/watch?v=Eyuguc7KKC4&feature=player_embedded#at=61 (Click here to see video)
Did you meet the objectives?? • Identify the stages of pressure ulcers • Identify patients at risk for pressure ulcers • Identify 3 ways to decrease risk and incidence of pressure ulcers (prevention) • Identify 3 complications of pressure ulcers Click the link if you want to review!
TRY AND RUN WITH IT Questions? Email jethandr@alverno.edu
References • Abrass, I., Kane, R., Ouslander, J. (2004). Essentials of Clinical Geriatrics. (5th ed.). McGraw Hill-Companies, Inc.Hightstown, NJ. • Agency for Health Care Policy and Research (2008). AHCPR Supported Guide and Guidelines [Internet]. Rockville: MD. Retrieved on April 2, 2011 from http://www.ncbi.nlm.nih.gov/books/NBK17977/. • Anders, J., Heinemann, A., Leffmann, C., Leutenegger, M., Profener, F., & Von-Rentein-Kruse, W. (2010). Decubitus Ulcers: Pathophysiology and Primary Prevention. Deutsches Arzteblatt International, 107 (21): 371-82. • Aurora Health Care (2010). Skin Integrity Alterations Potential/Actual for Adult Inpatients. Milwaukee, WI: Aurora HealthCare. • Bright Hub Inc. (2011). Healing Bedsores. Retrieved on April 2, 2011 from http://www.brighthub.com/health/alternativemedicine/articles/52007. aspx. • Capezuti, E., Fulmer, T., Mezey, M., & Zwicker, D. (2003). Evidenced Based Geriatric Nursing Protocols For Best Practice. (3rd ed). Springer Publishing Co., New York, NY. • Cassell, C. (2009). Pressure Ulcer Assessment: The Braden Scale for Predicting Pressure Ulcer Sore Risk. Health Services Advisory Group. • Guren, D. (2010). Skin is in: positioning your surgical patient matters. Retrieved March 28, 2011 from http://uwcne.net/grandrounds/display.asp?ID=48& submit=Video.