Download
1 / 33
330 likes | 613 Views
TUBERCULOSIS IN THE AGE OF HIV. Dr. Terry Baker Physician National Chest Hospital. THE PROBLEM. Global epidemic of HIV infection. HIV- infected persons highly susceptible to M. tuberculosis disease. Impact of HIV epidemic and TB greatest in the developing world.

E N D
TUBERCULOSIS IN THE AGE OF HIV Dr. Terry Baker Physician National Chest Hospital
THE PROBLEM • Global epidemic of HIV infection. • HIV- infected persons highly susceptible to M. tuberculosis disease. • Impact of HIV epidemic and TB greatest in the developing world. • 33% HIV infected population co-infected with TB. • TB - the most common opportunistic lung infection.
Tuberculosis & HIV Region Adults & Children Adult living with HIV/AIDS Prevalence Rate Sub-Saharan 23.3 million 8.0 % Latin America 1.3 million 0.57 % Caribbean 360,000 1.96% Western Europe 520,000 0.25% North America 920,000 0.56% World HIV/AIDS Statistics by Region, December 1999
New AIDS Cases Per Year Per 100,000 Population 35 Caribbean 30 25 20 North America 15 10 Latin America 5 0 2000 90 91 92 93 94 95 96
CO-INFECTION RATES Jamaica
TUBERCULOSIS AND HIV Implications: two-fold One epidemic (i.e. HIV) can potentially drive a second epidemic (i.e. Tuberculosis). Intersection of both epidemics could potentially spawn a third: i.e. Multiple Drug Resistant Tuberculosis ( MDRTb ).
Tuberculosis & HIV MDRTb : Tb resistant to conventional therapy: Isoniazid ( INH ) and Rifampicin Treatment regimen is six-seven drugs Mortality remains in excess of 80 % Has the potential to infect both HIV and non- HIV populations
Tuberculosis & HIV Conversion ( to active Tb disease after infection ) : Non-HIV : following infection, conversion is 5-10% over a lifetime HIV: conversion is 5-10% per year
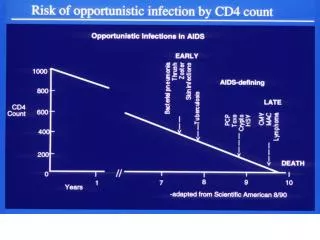
PATHOGENESIS OF CO-INFECTION • HIV-infected persons are at risk for primary or reactivated TB, and for second episodes of TB. • Reduced T1 response. • CD 4+ lymphocytes unable to produce alpha- interferon. • Alpha-interferon central to anti- mycobacterial immune defenses.
PATHOGENESIS OF CO-INFECTION • Presence of TB up-regulates retroviral replication. • TB infection produces proinflammatory cytokines. • Risk of death 2x greater in HIV-infected patients with TB. • Death due to progression of HIV and not TB.
CLINICAL PRESENTATION • Dependent on degree of immunosuppression. • Presentation varied. • Extra-pulmonary TB, particularly lymph node involvement more common.
Diagnosis • History- Malaise, weight loss, fever, cough, haemoptysis • Physical Examination • Laboratory Examinations – AFB smear, lymph node biopsy, BAL, pleural biopsy, cultures • Chest X-ray – findings variable • ? Mantoux Test • ? Rapid diagnostic tests- identifies TB RNA or DNA
HIV AND THE TREATMENT OF TUBERCULOSIS • Six months vs. Nine months • Clinical or bacteriological delayed response- Longer therapy. • Lack of adherence to therapy most important impediment to cure. • Higher risk of MDRTb • Greater risk of prolonged disease. • Strong public health services (DOT) improve outcome.
TREATMENT OF TUBERCULOSIS • First line drugs- Rifampin, Isoniazid, Pyrazinamide, Ethambutol, Streptomycin. • Rifampin- most important and most potent. • Second line drugs- Quinolones, Amikacin, Capreomycin.
ANTI-RETROVIRAL THERAPY • HAART dramatic improvement in prognosis for HIV- infected patients. • Drug interactions complicate the management of tuberculosis. • Interaction is mainly with the Rifamycins.
PHARMACOKINETICS OF ARV’S AND ANTI-TB DRUGS Rifamycins induce CYp450, decreasing serum levels of the protease inhibitors. Protease inhibitors inhibit CYp450 system, increasing serum rifamycins levels to possibly toxic levels. Net effect is that protease inhibitors may lose their efficacy and rifamycin toxicity may be increased.
PHARMACOKINETICS OF ARV’S AND ANTI-TB DRUGS • Rifampicin is the most potent inducer CYp450 • Rifabutin is the least potent inducer and may be substituted for rifampicin. • Clinical trials have demonstrated comparable safety and efficacy. • The dose of rifabutin should be reduced from 300 to 150 mg daily in pts. on Protease Inhibitors. • CDC. Report of the NIH panel to define principles of therapy of HIV infection and guidelines for the use of antiretroviral agents in HIV-infected adults and adolescents. MMWR 1998; 48 ( No. RR-5): 1 -63
PHARMACOKINETICS OF ARV’S AND ANTI-TB DRUGS Protease inhibitors that can be concurrently administered with Rifabutin are Indinavir and Nelfinavir. More recently: Lopinavir, Amprenavir can be given, but with adjusted doses of Rifabutin: 150mg daily.
PHARMACOKINETICS OF ARV’S AND ANTI-TB DRUGS NNRTI’s - may inhibit or induce p450. Efavirenz - rifabutin dosage should be increased. Nevirapine can be used without dosage adjustment. NRTI’s- Rifamycins can be used without dose adjustment.
PHARMACOKINETICS OF ARV’S AND ANTI-TB DRUGS Regimens with rifamycins are shorter, have faster conversion and lower relapse rates than those without. HIV-infected TB patients treated without rifamycins may have a higher risk of dying.
CONTROVERSIES • ? Continuation of anti-retroviral therapy during Anti-TB therapy. • ? Anti-TB regimens not including a rifamycin. • ? When to initiate anti-retroviral therapy in HIV-infected TB patient. • ? Risk of paradoxical reactions and glucocorticoid therapy. • ? Malabsorption of anti-TB meds.
PARADOXICAL REACTIONS • Up to 1/3 of co-infected patients on anti-Tb meds will experience paradoxical worsening when antiretroviral therapy is introduced. • The clinical manifestation is usually fever, intrathoracic and cervical lymphadenopathy, pleural effusions and/or skin lesions. • Usually occurs within 15 days of initiation of therapy. Paradoxical worsening of Tb following antiretroviral therapy in pts with AIDS Am. J Respir Crit Care Med 1998; Nariita M et al Smith H. Paradoxical responses during the chemotherapy of tuberculosis. J. Infect Dis 1987; 15: 1-3
PARADOXICAL REACTIONS • This appears to be associated with a marked drop in HIV viral load even though the peripheral CD4+ remains abnormally reduced • Paradoxical reactions have been attributed to strengthening of the host’s delayed hypersensitivity response, a decrease in suppressor mechanisms and / or an increased exposure to mycobacterial antigens following bactericidal TB chemotherapy
CHEMOPROPHYLAXIS FOR TB • Need to exclude active disease. • Recommended for recent close contact with potentially infectious persons with TB. • ? Positive Mantoux test and need for prophylaxis. • Isoniazid for nine months OR Rifampin/ Rifabutin & Pyrazinamide for two months.
THE FUTURE • Decline in the number of TB cases in persons with HIV due to better availability of ARV. • Development of new anti-Tb and ARV with fewer drug interactions essential to reduce morbidity and mortality. • Strengthened Public Health Services