Download
1 / 80
1.11k likes | 1.98k Views
RADIATION PROTECTION. Dr.P.P.Mohanan Thrissur. Outline. Basis for protection, radiation risk and recommendations Personal dosimetry Protection tools. Vulnerable Interventional Cardiologist. POTENNTIAL HAZARDS.

E N D
RADIATION PROTECTION Dr.P.P.Mohanan Thrissur
Outline • Basis for protection, radiation risk and recommendations • Personal dosimetry • Protection tools
Coronary interventionalists must also have a thorough knowledge of specialized equipment, techniques, and devices used to perform PCI competently
AHA Scientific Statement - 2014 Approaches to Enhancing Radiation Safety in Cardiovascular Imaging A Scientific Statement From the American Heart Association Recommendations All healthcare providers who can request cardiac imaging procedures should be required to know (a) which cardiac imaging tests use ionizing radiation; (b) basic concepts related to medical radiation exposure, including the concepts of absorbed dose and effective dose; and (c) typical dose estimates for the most commonly used cardiac imaging procedures (Class I; Level of Evidence C). All healthcare providers who will perform cardiac imaging with ionizing radiation, including interventional cardiologists and electrophysiologists, should be required to demonstrate adequate knowledge of contemporary dose-optimization techniques for patients and dose-minimization techniques for operators and staff (Class I; Level of Evidence C).
Recommendations 1.Education.of clinicians and patients 2.Justificationthat a particular cardiac imaging test with radiation is needed 3.Optimization of radiation exposure (choosing the smallest dose that provides high-quality images).
Importance of training • European Guidelines published in 2000. • Radiologists 30-50 hours • Cardiologists 20-30 hours • Other doctors using fluoroscopy X rays systems 15-20 hours Available at:http://europa.eu.int/comm/environment/radprot Lecture 6: Standards and guidance
Responsibilities Advice of qualified expert Cardiologist Patient Protection Training criteria Justification Optimization Equipment design and suppliers Quality assurance Lecture 6: Standards and guidance
Limits on Patient Doses? • There are no regulatory limits on the radiation dose a patient may receive • Question: do you think that the benefit outweighs the risk??? Lecture 6: Standards and guidance
Time of onset of clinical signs of skin injury depending on dose received • Symptoms Dose range Time of onset • (Gy) (day) • Erythema 3-10 14-21 • Epilation >3 14-18 • Dry desquamation 8-12 25-30 • Moist desquamation 15-20 20-28 • Blister formation 15-25 15-25 • Ulceration >20 14-21 • Necrosis >25 >21 • Ref.: IAEA-WHO: Diagnosis and Treatment of Radiation Injuries.
Scatter radiation X-Ray Lab Personnel Patient Operator Measures taken to reduce radiation exposure to patient will also benefit the operator/cath. lab. staff
Radiation risk • Stochastic effect • Deterministic effect
Deterministic vs. stochastic effects (representative, not scaled). Picano E et al. Eur Heart J 2014;eurheartj.eht394
Radiation effects Early (deterministic only) Late Local Radiation injury of individual organs: functional and/or morphological changes within hrs-days-weeks Common Acute radiation disease Acute radiation syndrome Deterministic Radiation dermatitis Radiation cataracta Teratogenic effects Stochastic Tumours Leukaemia Genetic effects
Deterministic effect • Gray is unit of exposure of radiation • ONE CHEST X RAY 0.15 mGRAY • 10000 chest x ray • Or • 100 CT abdomen = • 30 mins to 1 hr fluoroscopy exposure
0.5 – 2.5 mSv/h 1- 5 mSv/h 2- 10 mSv/h
Limits on Occupational Doses (ICRP)* *Please follow the recommendations as prescribed by your national authority
Threshold doses for some deterministic effects • 0,1 Gy– detectible opacities • 0,2 Gy– sterility for woman • 0,4 Gy– visual impairment • 0,4 Gy– temporary sterility for man • 0,4Gy– depression of haematopoiesis • 1,0Gy– chronic radiation syndrome • 2,0 Gy – permanent sterility for man
Radiation dose in coronary angiography and Intervention: Journal of Medical Radiation Sciences
A Typical Fluoroscopic Lab Overhead shields need to be positioned down next to the patient and adjacent to the image intensifier to seal scatter off from below. Table skirts shield the highest backscatter levels from the x-ray tube.
To obtain the images … • Two technologies are used: • Image intensifier • Flat panel detector
The X-ray Imaging Process Absorption and transmission of x-rays contribute to the imaging process and patient dose. Scattered or partially absorbed x–rays contribute to occupational exposure, but are less than 1% of the primary beam intensity.
Comparison of Philips H 3000 and Innova 2000 in PCICharacteristics of procedures & lesions %
Recommendations 1.Education. of clinicians and patients 2.Justification that a particular cardiac imaging test with radiation is needed 3.Optimization of radiation exposure (choosing the smallest dose that provides high-quality images).
Basic Radiation Safety Techniques Time - As exposure time increases, dose accumulates -- Keep fluoro times as short as possible. A bell or buzzer will go off after 5 minutes of beam time, keep track of fluoro time, Distance - As distance from the radiation source increases, the radiation intensity decreases rapidly -- Keep patient anatomy and staff as far away from the x-ray tube port as possible Shielding - Diagnostic x-rays are easily shielded with thin sheets -- Wear lead aprons, thyroid shields, leaded glasses and use overhead leaded shields and table skirts
Optimization means ... • To avoid acquiring more images than necessary: • Take care of the fluoroscopy time. • Take care of the number of series. • Take care of the number of frames per series. • To avoid acquiring images with more quality (and more dose) than necessary: • It could be possible to accept sometimes some noisy images in fluoroscopy and also in cine acquisitions.
ALARA rule • As low as reasonably achievable • Reduce number of exam • Reduce time of exam • Use alternaive
Minimize Exposure Time • Everything you do to minimize exposure time reduces radiation dose!! • Minimize fluoro and cine times • Whenever possible, step out of room • Step behind barrier (or another person) during fluoro or cine • Use pulsed fluoroscopy– minimizes time X ray tube is producing X rays
Siemens Axiom Artis, Fluoro low dose 20 cm PMMA 13 Gy/fr (entrance PMMA) Siemens Axiom Artis Cine normal mode 20 cm PMMA 177 Gy/fr (entrance PMMA)
The proposed reference levels for Coronary Angiography and PTCA were DAP 45 Gy•cm2 and 75 Gy•cm2; fluoroscopy time 7.5 min and 17 min and number of frames 1250 and 1300, respectively. Lecture 9: Optimization of Radiation Protection in Cardiology
Influence of operation modes: from low fluoroscopy to cine, scatter dose rate could increase in a factor of 10 (from 2 to 20 mSv/h for normal size)
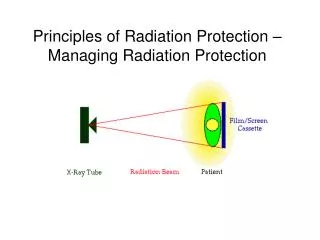
The inverse square law Source Because the same energy is spread over a surface 4 times larger at a doubled distance, the same object will receive only a fourth of the dose when moved away from “d” to “2d” d 2d Doubling the distance from the source divides the dose by a factor of 4
Collimators use in reduce exposure FOV 15 dose reduction 25%
Collimators reduce exposure FOV 20
Anti-scatter grid Increase DAP and skin dose x 2 times Improve image quality
FILTERING improper filtering causes image deterioration proper filtering Filtering prevents image saturation in low absorption areas
Optimization requires………. • Knowledge of factors contributing to patient and staff radiation dose • patient factors • procedural factors • equipment (machine) factors • Knowledge of dose reduction capabilities of our X ray system • Periodic update of our clinical and technical working protocols
Optimization is especially important in more complex PTCA procedures • chronic total occlusion • bifurcation lesion • degenerated saphenous vein graft lesion • lesion in severely tortuous vessel • ostial lesion
Exposure variation in exposure rate (DAP rate) with projection Cusma JACC 1999